
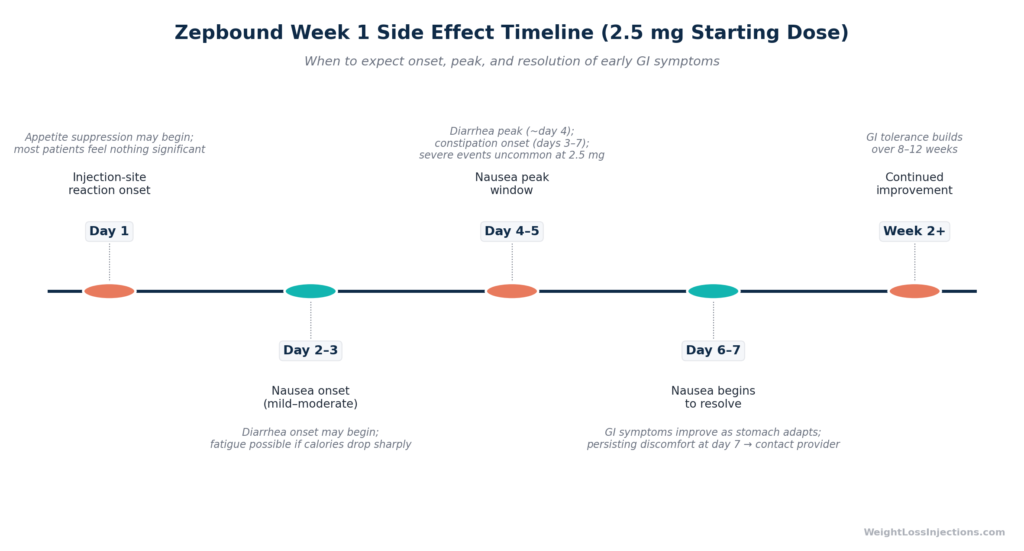
Zepbound Week 1 Side Effect Timeline (2.5 mg Starting Dose)
The first week on Zepbound is where expectation and reality most often diverge, and usually in a reassuring direction. The 2.5 mg starting dose is a deliberate tolerability step, not yet a therapeutic dose, meaning GI side effects are at their lowest possible intensity. For most patients, nausea onset comes days 2–3, peaks around days 4–5, and begins resolving by day 6–7. The Zepbound prescribing information reports a lifetime nausea rate of 25–29% across maintenance doses, but the 2.5 mg starting experience is meaningfully milder.
Understanding the timeline, and the difference between expected discomfort and a genuine red flag, is what week 1 preparation actually requires.
What the FDA Data Says About Week 1 Side Effects
Adverse Event Rates from Clinical Trials (Studies 1 & 2, Pooled)
The most reliable reference point for Zepbound side effects is the adverse event table from the Zepbound prescribing information, Table 1, which pools data from Studies 1 and 2, the two SURMOUNT trials that formed the basis for FDA approval on November 8, 2023, per the FDA press release.
The pooled rates across all maintenance doses (5 mg, 10 mg, 15 mg) versus placebo:
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea† | 8% | 19% | 21% | 23% |
| Constipation‡ | 5% | 17% | 14% | 11% |
| Vomiting | 2% | 8% | 11% | 13% |
†Includes diarrhea and frequent bowel movements. ‡Includes constipation and feces hard.
Source: Zepbound prescribing information, Table 1
These are lifetime-of-treatment averages — not week-1 rates. Two important context points from the label:
- GI adverse reactions occurred in 56% of pooled Zepbound patients vs. 30% placebo, but this counts any GI event at any point during 72 weeks of treatment.
- Severe GI adverse events were uncommon even at the highest dose: 1.7% at 5 mg, 2.5% at 10 mg, and 3.1% at 15 mg, versus 1.0% for placebo — per Zepbound prescribing information.
The SURMOUNT-1 trial in the New England Journal of Medicine (Jastreboff et al., 2022) established that GI adverse events were heavily concentrated in the early weeks of treatment — particularly in the first 4 weeks after the first injection and after each subsequent dose escalation. As patients remained on a stable dose, GI event rates declined substantially. Week 1 is the highest-burden window of the entire treatment course at that dose level, which is both the worst news and the best news: it will not be this difficult again unless you escalate.
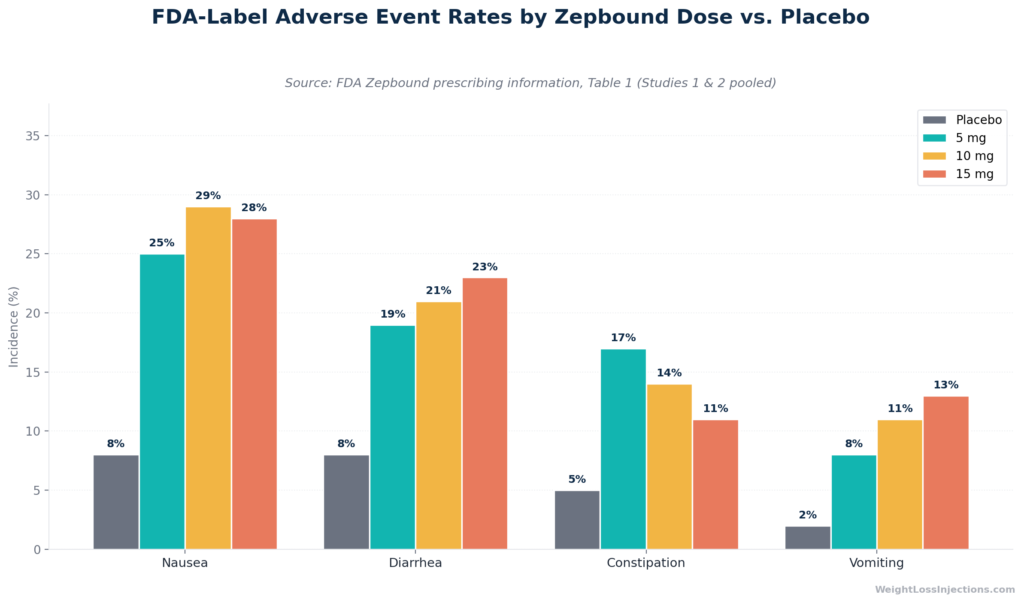
FDA-Label Adverse Event Rates by Zepbound Dose vs. Placebo
The 2.5 mg Starting Dose: Intentionally the Lowest Burden
The Zepbound prescribing information, dosing section is explicit: the 2.5 mg once-weekly starting dose is a tolerability step only — it is not an approved maintenance dose. The full titration sequence is 2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg, with each step lasting a minimum of 4 weeks. Total time to reach 15 mg is a minimum of 20 weeks.
This design is deliberate. Tirzepatide is a dual GIP/GLP-1 receptor agonist, and the primary mechanism driving GI side effects — slowed gastric emptying, altered gut motility — is dose-dependent. Starting at 2.5 mg exposes GIP and GLP-1 receptors to the minimum pharmacologically active concentration, allowing the gastrointestinal system to begin adapting before the dose reaches therapeutic levels.
What does this mean practically? Patients starting Zepbound for the first time at 2.5 mg will experience the lowest GI burden they will encounter at any point during treatment. The adverse event rates in the FDA label’s pooled data (nausea 25–29%, diarrhea 19–23%) are generated almost entirely at maintenance doses of 5 mg and above. Most patients who describe week 1 as manageable, and most do, are describing the 2.5 mg experience specifically.
Tirzepatide has an elimination half-life of approximately 5–6 days per the Zepbound prescribing information, which means peak plasma concentration (Tmax) occurs 8–72 hours after subcutaneous injection and the drug remains pharmacologically active throughout the entire week. The GI effects patients experience in week 1 are the result of this sustained receptor engagement, not a bolus effect that clears within a day.
Day-by-Day Timeline: What Patients Experience in Week 1
The following timeline synthesizes the FDA label’s adverse event data with the GI event timing patterns documented in SURMOUNT-1 (Jastreboff et al., NEJM 2022). Day numbers are approximate; individual variation is real and normal.
Day 1 (Injection Day)
Most patients feel nothing beyond mild injection-site effects in the hours immediately following their first Zepbound dose. Per the Zepbound single-dose pen Instructions for Use, injection-site reactions, redness, itching, mild swelling, or brief stinging — can appear within 1–2 hours at the injection site and typically resolve within 24–48 hours without intervention.
Appetite suppression may begin within hours of injection as tirzepatide engages GIP and GLP-1 receptors, which regulate satiety signaling through gastric emptying delay and central appetite pathways. This is not a side effect to manage, it is the mechanism working. Patients often describe day 1 as unremarkable, with the primary sensation being a modest reduction in hunger.
Significant nausea, diarrhea, or vomiting on day 1 is uncommon at 2.5 mg. If you experience severe symptoms within hours of your first injection, contact your provider, this timing may indicate a hypersensitivity reaction rather than standard GI adaptation.
Days 2–3
Days 2 and 3 are when the most commonly reported GI symptom, nausea, typically begins. The mechanism is straightforward: tirzepatide slows gastric emptying through GLP-1 receptor activation, and the stomach, which is not yet adapted to this altered rhythm, interprets delayed emptying as a signal resembling nausea. At 2.5 mg, this effect is mild to moderate for most patients.
Diarrhea may begin in this window. Like nausea, it reflects altered GI motility, in this case, GLP-1 receptor activity in the intestine affecting transit time. Not every patient experiences diarrhea; the 5 mg pooled rate of 19% from the Zepbound prescribing information is a ceiling figure, and 2.5 mg rates are expected to be lower.
Fatigue is a reported adverse event in Zepbound’s clinical program per the FDA press release (November 8, 2023). It can emerge in days 2–3 if reduced appetite leads to sharply decreased caloric intake, the body adapting to lower energy availability. Maintaining adequate nutrition despite appetite suppression is important during this window.
Days 4–5 (Peak Side Effect Window)
This is the highest-burden period of week 1. Nausea typically peaks in the days 2–5 window per the synthesis of SURMOUNT-1 timing data; the majority of patients who experience it reach their worst point somewhere in days 4–5. At 2.5 mg, most patients describe this as an annoying nausea, present but manageable, rather than incapacitating.
If diarrhea is occurring, it tends to peak around day 4. Constipation, which has a different onset trajectory, may begin manifesting in the day 3–7 window per the Zepbound prescribing information; constipation represents the opposite motility effect from diarrhea, and it often follows rather than accompanies diarrhea in the early weeks.
Abdominal pain and discomfort, also listed in the FDA approval language per the FDA press release — can accompany the peak GI window. Typically this is cramping or fullness rather than sharp pain. Sharp pain, particularly pain radiating to the back or upper right quadrant, is a red flag requiring immediate provider contact (see Red Flags section below).
Severe GI events at the 2.5 mg starting dose are uncommon. Even at 5 mg — the lowest maintenance dose — the rate of severe GI adverse events was only 1.7% in SURMOUNT-1 pooled data per the Zepbound prescribing information. Most patients at 2.5 mg can function normally through days 4–5 with appropriate dietary management.
Days 6–7
For the majority of patients, days 6 and 7 mark the beginning of GI symptom resolution. Nausea begins to ease as the stomach progressively adapts to slowed gastric emptying. The physiological adaptation process, GI receptors developing tolerance to tirzepatide’s motility effects, is active throughout week 1 and continues beyond it.
The SURMOUNT-1 findings (Jastreboff et al., NEJM 2022) are consistent with this: most GI adverse events in the first 4 weeks were transient, and discontinuation due to GI adverse events was uncommon in the 2.5–5 mg window.
If you are still experiencing significant nausea or other GI symptoms at day 7, this is not a sign that treatment is failing — it is information for your provider. Per the Zepbound prescribing information’s dosing guidance, patients who do not tolerate dose escalation may remain at any dose for an additional 4 weeks before attempting titration. Staying at 2.5 mg for a second 4-week period is a clinically valid option. Contact your provider rather than stopping independently.
What’s Different: First Injection vs. Dose Escalation Week 1
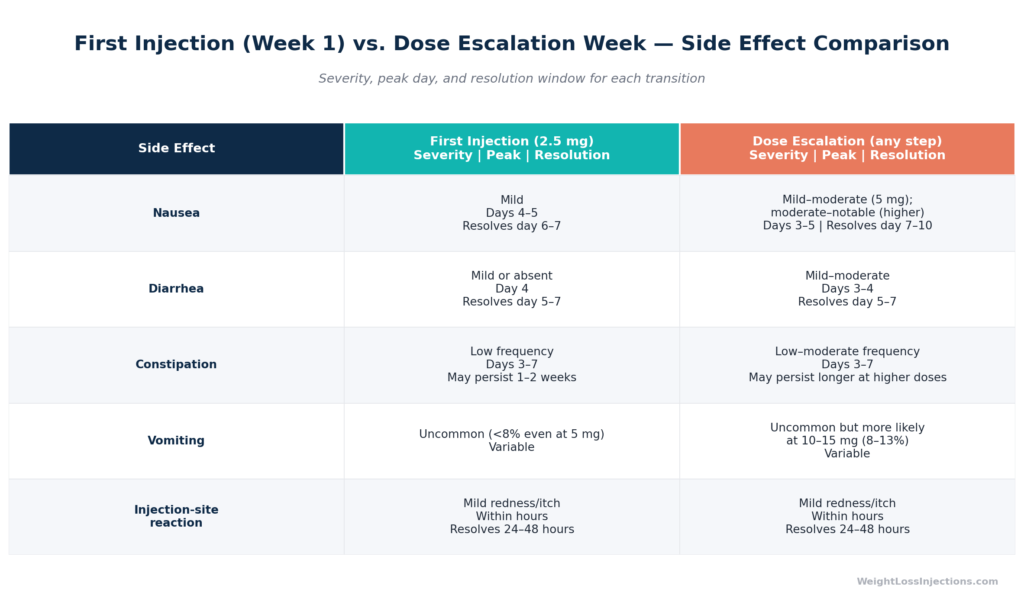
First-Ever Injection at 2.5 mg
At your first Zepbound injection, two factors combine to produce the lowest side-effect burden you will experience during treatment. First, your GIP and GLP-1 receptors are naive, they have not been exposed to tirzepatide before, but this is offset by the second factor: 2.5 mg is the lowest dose in the titration sequence, and the GI effects of tirzepatide are dose-dependent.
Patients who describe week 1 as entirely manageable, some report no GI symptoms at all, are disproportionately describing the first-injection 2.5 mg experience. The Zepbound prescribing information does not publish a separate 2.5 mg adverse event table because the tolerability dose is not a maintenance dose, but the dose-response relationship evident from the 5 mg, 10 mg, and 15 mg data (nausea 25%, 29%, 28% respectively) strongly suggests 2.5 mg rates sit meaningfully below 25%.
Patients in this first week should not interpret “it was easier than I expected” as evidence that the medication isn’t working. Appetite suppression, the mechanism that drives weight loss, begins at 2.5 mg. The scale may not yet reflect meaningful change, but the biology is underway.
First Week After a Dose Escalation
Each dose increase, 2.5 mg to 5 mg, 5 mg to 7.5 mg, and every subsequent step, triggers a new wave of GI side effects in the days following the first injection at that dose. This is a “mini week 1 reset,” and it is expected and documented. The higher the new dose, the more pronounced this effect can be.
The dose-response relationship is clear from the Zepbound prescribing information, Table 1: nausea rises from 25% at 5 mg to 29% at 10 mg before slightly declining at 15 mg (28%); vomiting increases more linearly from 8% (5 mg) to 13% (15 mg). Patients escalating to higher doses should anticipate a side-effect burden meaningfully greater than their first week at 2.5 mg.
The critical difference: at escalation steps, patients already have baseline GI tolerance to tirzepatide from weeks of prior exposure. While the new dose resets the intensity of GI effects temporarily, the body is not starting from zero, the GI tract has adapted to the drug’s mechanism, just not yet to the higher concentration. For most patients, escalation-week side effects are manageable and resolve within 7–10 days, at which point adaptation resumes.
Per the Zepbound prescribing information: the minimum interval between dose increases is 4 weeks. Escalating faster than this does not allow adequate GI adaptation time and substantially increases side-effect burden.
Managing Week 1 Side Effects: What Actually Helps
Dietary Adjustments (Most Impactful)
The most effective intervention for Zepbound week 1 nausea is dietary modification. Tirzepatide slows gastric emptying; large, rich, or fatty meals sit in the stomach longer than normal, amplifying nausea through mechanical distension and altered motility. The solution is reducing meal volume and fat load.
Eat 4–6 small meals per day and stop at 70–80% of your normal fullness. This is not a weight-loss strategy for week 1 — it is a tolerance strategy. The Zepbound.lilly.com nausea management guidance mirrors this approach: reduce portion sizes and avoid high-fat foods, particularly during the peak side-effect window of days 2–5.
Foods that are well-tolerated during week 1 GI symptoms: plain rice, plain toast, bananas, crackers, clear broth, boiled or steamed plain vegetables. Foods to avoid during peak days: fried foods, fatty meats, rich sauces, alcohol, and spicy dishes. These categories are referenced in Eli Lilly’s official patient guidance and align with the dietary guidance in the Zepbound prescribing information.
Eating slowly and not lying down for at least 30–60 minutes after meals also reduces nausea burden by allowing gastric emptying to proceed without the additional complication of positional reflux.
Hydration
Maintaining adequate hydration is not optional during week 1, it is clinically important. The Zepbound prescribing information explicitly identifies dehydration caused by GI adverse reactions (nausea, vomiting, diarrhea) as a mechanism for acute kidney injury (AKI). This is listed under “Warnings and Precautions.”
Aim for 8–10 glasses of still water daily. If you experience vomiting or diarrhea in week 1, increase intake accordingly and use electrolyte replacement (oral rehydration solutions) if losses are significant. The warning about AKI is not intended to alarm patients about mild nausea, it is a guide for managing the uncommon but serious scenario where GI losses are severe enough to cause dehydration over multiple days. If you cannot keep fluids down for more than 24 hours, contact your provider the same day.
Carbonated beverages can worsen nausea by increasing gastric distension; still water or herbal teas are preferable during peak symptom days.
Injection Timing
Some patients report better GI tolerance when injecting Zepbound at night, shortly before sleep. The rationale is straightforward: peak plasma concentration (Tmax) occurs 8–72 hours after injection per the Zepbound prescribing information, and shifting injection to bedtime means the early nausea onset, days 2–3, may fall during sleep or quieter periods rather than during work or active daytime hours.
This is a patient-reported strategy, not a clinical directive. The Zepbound prescribing information states that Zepbound can be injected at any time of day, with or without food. Consistency matters more than timing: irregular weekly injection intervals can produce concentration fluctuations that intensify GI effects. Stick to the same day and, if helpful, the same time.
Injection site rotation is also important. Per the Zepbound single-dose pen Instructions for Use, inject into the abdomen (stomach), outer thigh, or back of upper arm, rotating sites weekly. Do not inject into the same site consecutively.
OTC Options (With Provider Guidance)
Several over-the-counter medications are sometimes used for week 1 GI symptom management. These should be discussed with your provider before use:
- Nausea: Meclizine (Dramamine Less Drowsy) or ginger supplements (ginger tea, ginger chews) are commonly used. Meclizine is an antihistamine-based antiemetic; while not specifically studied with tirzepatide, it does not have known direct interactions. Ginger has evidence for mild antiemetic benefit. Confirm OTC use with your provider before starting.
- Diarrhea: Loperamide (Imodium) may be appropriate for acute loose-stool episodes on a short-term basis. Do not use routinely or for extended periods without provider guidance.
- Constipation: Docusate (Colace) is a gentle stool softener appropriate for early-onset constipation in week 1. Bulk-forming agents such as psyllium (Metamucil) are also useful but are better introduced after the initial diarrhea risk window has passed, as adding fiber during acute diarrhea can worsen symptoms.
Your provider, whether clinic-based or telehealth, can advise on which options are appropriate given your full medication list and health history. Do not use anti-nausea prescription medications without provider authorization.
Red Flags: When to Call Your Provider Immediately
The vast majority of week 1 side effects on Zepbound at 2.5 mg are self-limiting and managed at home. The following symptoms are not expected discomfort — they require same-day provider contact or emergency evaluation:
Inability to keep fluids down for more than 24 hours. Persistent vomiting preventing hydration creates acute kidney injury risk, per the Zepbound prescribing information’s AKI warning. This is not a “push through it” scenario.
Severe abdominal pain radiating to the back. This symptom pattern is a potential indicator of acute pancreatitis. The Zepbound prescribing information lists pancreatitis as a serious warning and precaution: discontinue Zepbound if pancreatitis is suspected and do not restart without provider evaluation. Pancreatitis can be fatal if untreated.
Upper right quadrant abdominal pain, fever, or jaundice. This triad suggests potential gallbladder disease — cholelithiasis or cholecystitis. The Zepbound prescribing information lists gallbladder disease as a warning and precaution: notify your healthcare provider if these symptoms develop.
Severe, worsening symptoms that do not improve by day 7. GI symptoms at 2.5 mg should begin resolving by the end of week 1. Symptoms that are escalating rather than resolving at day 7 warrant clinical evaluation rather than continued home management.
Signs of serious hypersensitivity reaction. Per Zepbound’s contraindications, Zepbound is contraindicated in patients with known serious hypersensitivity to tirzepatide. Symptoms of anaphylaxis or angioedema, rash or hives, swelling of the face or throat, difficulty breathing, rapid heartbeat, or dizziness, require emergency evaluation (call 911 or go to an emergency room). These reactions are uncommon but can occur with any injection and are not the same as the expected GI side effects of treatment.
One additional note: do not use Zepbound concurrently with Mounjaro or any other GLP-1 receptor agonist (semaglutide, liraglutide, dulaglutide, or exenatide). Both Zepbound and Mounjaro contain tirzepatide; concurrent use creates an overdose risk. Per the FDA press release, this combination is explicitly prohibited.
What Week 1 Does NOT Predict
Week 1 Side Effects ≠ Long-Term Tolerability
A difficult week 1 does not predict a difficult month 6. This is one of the most important, and underemphasized, facts about starting Zepbound.
The SURMOUNT-1 trial (Jastreboff et al., NEJM 2022) showed that GI adverse events were heavily concentrated in the early weeks of treatment; the 72-week trial data show a steep decline in GI event rates as patients remained on a stable dose. Discontinuation due to GI adverse events was uncommon overall, the most frequent reason for discontinuation in SURMOUNT-1 was nausea (occurring in <5% of patients at the 5 mg dose as a reason for stopping), and the data consistently show that patients who stayed with the medication through the early weeks tolerated it well long-term.
Conversely, a smooth week 1 does not mean all dose escalations will be equally smooth. Each upward titration step brings a brief recurrence of GI side effects that follows the same week-1 pattern at a new intensity ceiling. Being prepared for each escalation prevents surprises.
The key insight: if you experience nausea, diarrhea, or fatigue in week 1, you are experiencing what was predicted in the clinical trial program and documented in the FDA label. It is not evidence that the medication is wrong for you. What matters is the trajectory, improving by days 6–7, even modestly, is the expected signal.
Week 1 Weight Loss Is Minimal — That’s Normal
The 2.5 mg tolerability dose is not designed to produce clinically meaningful weight loss. Weight loss on Zepbound begins in earnest when doses reach the therapeutic range, 5 mg and above, and the SURMOUNT-1 NEJM data (Jastreboff et al., 2022) show meaningful reductions of −15.0% at 5 mg, −19.5% at 10 mg, and −20.9% at 15 mg at 72 weeks — but these are long-term outcomes, not week-1 results.
In week 1, appetite suppression begins, and patients often experience a modest reduction in caloric intake. The scale may show a small downward movement, some of which reflects reduced food and fluid volume in the GI tract rather than true fat loss. Do not interpret a small number or no change at week 1 as evidence that the medication is not working. The pharmacology requires weeks at therapeutic doses to produce meaningful adipose tissue reduction.
Meaningful results from Zepbound emerge at 4–8 weeks of treatment at maintenance doses, not within the first week of the tolerability starting phase.
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: Week 1 on Zepbound is manageable for most patients, but “manageable” is not the same as “unguided.” The difference between a smooth first week and an unnecessarily uncomfortable one is almost always preparation: knowing the day-by-day timeline, modifying diet proactively before symptoms peak on days 4–5, staying ahead on hydration, and having a provider available to distinguish expected discomfort from a genuine red flag.
At WeightLossInjections.com, our licensed providers walk every patient through injection protocol, week-1 management, and titration planning before the first dose is administered, for [$X/month] covering [service detail]. You do not need to navigate the learning curve of a new medication without clinical support. Take our free eligibility quiz at WeightLossInjections.com to connect with a provider and start your titration with the right foundation.
Frequently Asked Questions
What are the most common Zepbound side effects in week 1?
The most common Zepbound side effects in week 1 are nausea, diarrhea, constipation, and fatigue. At the 2.5 mg starting dose, these are typically mild to moderate in intensity. Per the Zepbound prescribing information, Table 1, nausea affects 25–29% of patients at maintenance doses (5–15 mg); the 2.5 mg starting-dose rate is expected to be lower. Injection-site reactions, redness, mild pain, itching, are also common on day 1 and resolve within 24–48 hours. Most patients at 2.5 mg describe week 1 symptoms as present but manageable.
When does nausea peak after the first Zepbound injection?
Nausea from Zepbound typically begins on days 2–3 after injection, when tirzepatide concentrations are rising toward peak levels. The highest-intensity window is generally days 4–5, and most patients at 2.5 mg begin experiencing improvement by days 6–7. Tirzepatide’s half-life of approximately 5–6 days means plasma concentrations remain elevated throughout week 1, per the Zepbound prescribing information, which is why nausea does not resolve on day 2 or 3 — the drug is still at or near peak concentration.
Is it normal to feel no side effects in week 1 on Zepbound?
Yes. Not every patient experiences GI side effects at the 2.5 mg tolerability dose, and absence of symptoms does not mean the medication is not working. The FDA label adverse event rates for nausea (25–29%) and diarrhea (19–23%) are lifetime-of-treatment averages at maintenance doses per the Zepbound prescribing information, they do not represent week-1 incidence at 2.5 mg specifically. Patients who sail through week 1 without GI symptoms should still be prepared for increased side effects when dose escalation begins at week 5.
How long does Zepbound week 1 nausea last?
For most patients at the 2.5 mg starting dose, nausea begins resolving by days 6–7 and largely resolves within 7–10 days. The SURMOUNT-1 trial data (Jastreboff et al., NEJM 2022) consistently showed that GI adverse events were transient and concentrated in the first 4 weeks, after which rates declined substantially. Nausea that persists beyond day 7 without any improvement is not typical at 2.5 mg and should be discussed with your provider — you may benefit from an extended 4-week period at the starting dose before escalating.
What should I do if week 1 side effects are severe?
Contact your provider. Severe GI symptoms, defined as inability to keep fluids down for more than 24 hours, severe abdominal pain, or symptoms that significantly impair daily functioning, are not expected at 2.5 mg and warrant clinical evaluation. Per the Zepbound prescribing information’s Warnings and Precautions section, pancreatitis (severe pain radiating to the back), AKI risk from dehydration, and gallbladder disease (upper right quadrant pain with fever or jaundice) are serious events requiring prompt attention. Do not stop Zepbound independently without provider guidance — your provider may recommend dose delay, dietary modification, or clinical evaluation depending on your specific symptoms.
Do Zepbound side effects get worse with each dose increase?
Generally yes, in the short term. Each dose escalation triggers a temporary recurrence of GI side effects as the body adapts to a higher concentration of tirzepatide. The dose-response relationship is evident in the Zepbound prescribing information’s Table 1: vomiting rates increase from 8% at 5 mg to 13% at 15 mg, and severe GI adverse events increase from 1.7% at 5 mg to 3.1% at 15 mg. However, patients entering each escalation already have baseline GI tolerance from prior weeks of treatment, which moderates the intensity. Crucially, within 1–2 weeks at the new dose, GI symptoms typically resolve to a new (lower) baseline, so the “week 1” pattern repeats but does not continuously worsen throughout treatment.
This article is for educational purposes only and does not constitute medical advice. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. If you are considering Zepbound or any GLP-1 medication, consult a licensed provider about your individual history and circumstances.