
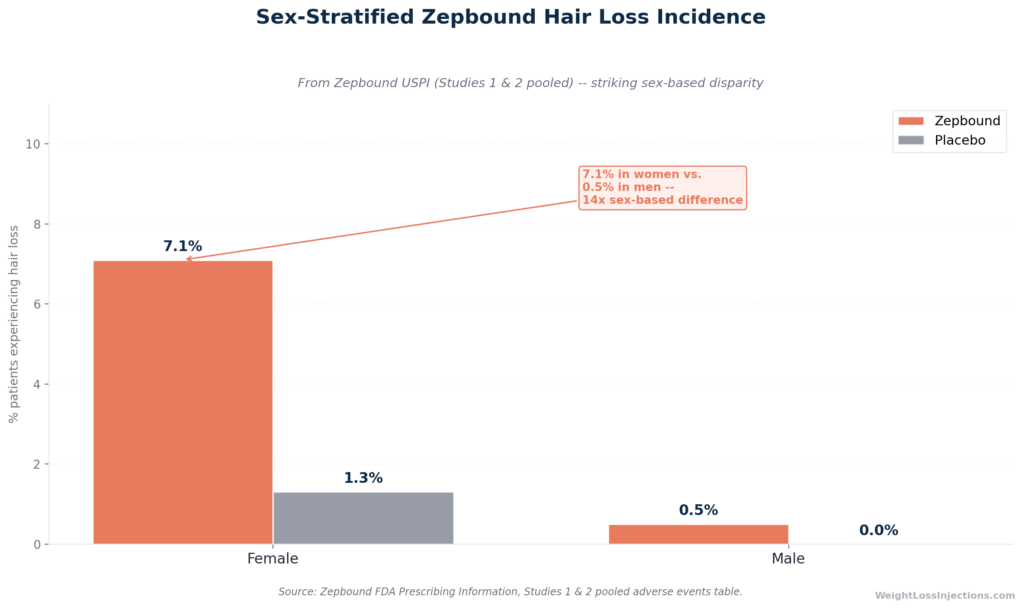
Sex-stratified Zepbound hair loss incidence (hero bar chart)
Hair loss is listed in the Zepbound FDA prescribing information as a real adverse event, occurring in approximately 5% of pooled clinical trial patients versus 1% on placebo, and in 7.1% of women specifically. But the mechanism is not direct drug toxicity. Zepbound drives rapid, substantial weight loss, and that weight loss triggers a well-characterized, reversible hair-shedding phenomenon called telogen effluvium.
Hair shedding typically begins 2–4 months into treatment, peaks over 1–3 months, and resolves on its own for most patients as weight loss decelerates. With adequate protein intake and targeted nutritional monitoring, the severity can be meaningfully reduced.
Safety notice: This article is for informational purposes only and does not constitute medical advice. If you are experiencing significant or persistent hair loss, consult a licensed dermatologist or your prescribing provider to rule out other causes.
What the Zepbound FDA Label Actually Says About Hair Loss
Hair loss is not a rumor, a social media complaint, or an off-label concern. It is a documented adverse reaction in the Zepbound FDA prescribing information, classified under the additional adverse reactions occurring in ≥2% of patients and at greater frequency than placebo.
The label data, drawn from the pooled weight reduction and long-term maintenance trials (Studies 1 and 2), show the following:
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Hair loss | 1% | 5% | 4% | 5% |
Source: Zepbound prescribing information, Table 1
The pooled active-treatment rate is approximately 5.7% across all Zepbound doses versus 1% on placebo — a roughly fivefold excess. That is enough to be clinically meaningful for patients planning treatment.
The Sex-Stratified Data Competitors Are Missing
The Zepbound label contains a finding that most patient-facing resources have ignored entirely: hair loss was dramatically more common in women than in men. From the Zepbound USPI adverse reactions section:
- Zepbound-treated patients: 7.1% of females vs. 0.5% of males
- Placebo patients: 1.3% of females vs. 0.0% of males
This is not a small numerical difference — it is a 14-fold sex disparity in the active treatment arm. Female patients on Zepbound experience hair loss at a rate more than 5 times higher than female placebo patients, while male patients on Zepbound appear barely distinguishable from male placebo patients at these pooled rates.
Importantly, no Zepbound-treated patients discontinued the study due to hair loss, indicating that while the symptom is common — especially in women — it did not reach severity levels requiring treatment discontinuation in clinical trials (Zepbound prescribing information).
How Zepbound’s Rate Compares to Bariatric Surgery
The critical context for interpreting these numbers: patients undergoing bariatric surgery, who experience comparable or greater rates of rapid weight losss, develop hair loss at rates of approximately 57% (95% CI 42–71%), according to a 2021 systematic review and meta-analysis in Obesity Surgery (PMC). That 57% figure dwarfs the 5–7% rates seen with Zepbound. The comparison does not minimize Zepbound-related hair loss, but it firmly establishes that rapid weight loss, not tirzepatide specifically, is the dominant driver.
The Hair Growth Cycle: Why Rapid Weight Loss Causes Shedding
To understand why hair loss happens on Zepbound and why it is reversible, you need a working mental model of how hair grows.
The Three Phases of Hair Growth
The scalp contains approximately 85,000–100,000 individual hair follicles at any given time, each cycling through three distinct phases independently of its neighbors (Zepbound prescribing information):
- Anagen (growth phase): Lasts 2–6 years. At any given time, approximately 85–90% of scalp hairs are in this phase, actively growing at a rate of roughly 0.5 inches (1.25 cm) per month.
- Catagen (transition phase): A brief 2-week period during which the follicle detaches from its blood supply. Approximately 1% of hairs are in catagen at any time.
- Telogen (resting/shedding phase): Lasts approximately 3 months. Roughly 10–15% of hairs are in this phase at any time. Normal daily shedding of 50–100 hairs represents telogen hairs being shed at their expected time.
The key insight is that these phases are staggered across your follicles, which is precisely why healthy individuals do not experience noticeable thinning despite shedding up to 100 hairs per day.
What Telogen Effluvium Is — and Isn’t
Telogen effluvium (TE) is a specific, well-characterized pattern of diffuse hair shedding that occurs when a significant physiological stressor, rapid weight loss, surgery, illness, childbirth, or severe caloric restriction, forces a large cohort of hair follicles to simultaneously exit the growth phase and enter the resting/shedding phase prematurely. According to a 2024 retrospective study of 140 TE patients in the Annals of Dermatology (PMC), TE induced by weight loss typically occurred when patients lost a mean of 15.21% of their body weight or shed approximately 3.54 kg per month, thresholds that Zepbound patients often exceed at higher doses.
When an unusually large percentage of follicles enter telogen simultaneously, the predictable consequence arrives 2–4 months later: those follicles shed together, producing visible diffuse thinning rather than the gradual, imperceptible shedding of a healthy scalp. The follicles themselves are not damaged. The papilla, the root of each follicle, remains intact. Regrowth begins as follicles cycle back into anagen once the triggering stress resolves.
What telogen effluvium is not: It is not androgenetic alopecia (male or female pattern baldness), which involves permanent follicle miniaturization. It is not alopecia areata, which involves autoimmune follicle destruction. And critically, it is not evidence that Zepbound is chemically damaging your hair. The Brazilian Journal of Hair Health review of TE in modern weight-loss therapies confirms this distinction: the mechanism is systemic metabolic stress, not drug-specific toxicity.
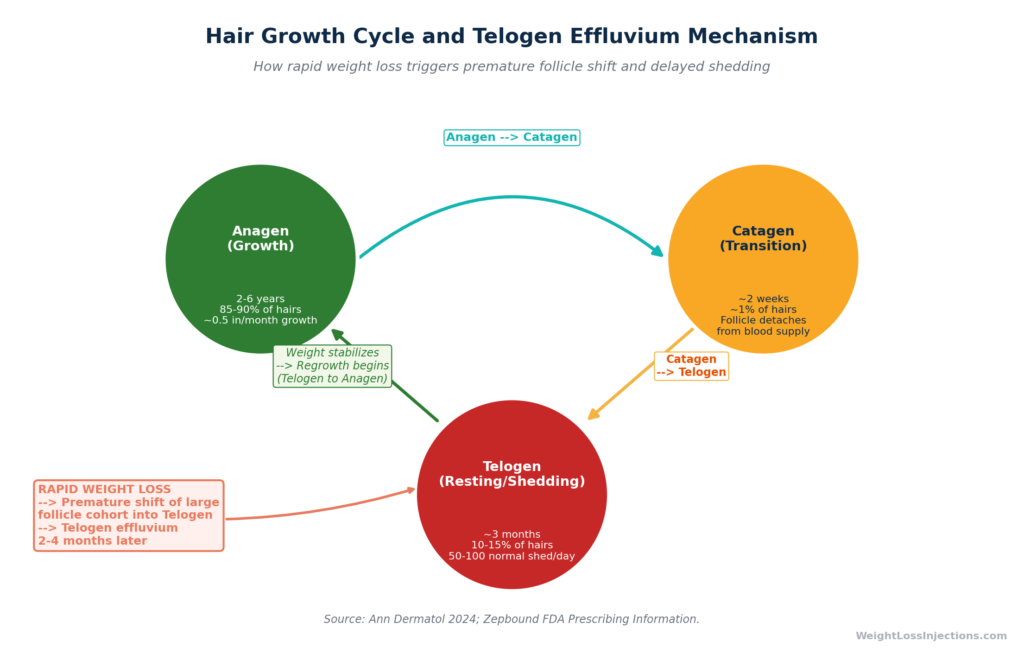
Hair growth cycle diagram
Why Zepbound Users Are Particularly Susceptible
Zepbound’s clinical efficacy, the reason it is prescribed, is also the primary driver of its hair loss risk. In SURMOUNT-1, patients on 15 mg tirzepatide lost a mean of 20.9% of body weight at 72 weeks, with the heaviest losses concentrated in the first 12–20 weeks of treatment (SURMOUNT-1, NEJM 2022). Those early months are precisely the window when hair follicles receive the physiological signal to shift into telogen — meaning the onset window for hair shedding (months 2–5 of treatment) aligns directly with the period of most rapid weight reduction.
There is a second mechanism layered on top of the weight-loss trigger: nutritional insufficiency. Zepbound’s dual GIP/GLP-1 receptor agonism substantially reduces appetite and food intake (Zepbound prescribing information). Patients who eat less overall, even with healthy intentions, risk reducing intake of protein, iron, zinc, and biotin below the minimum required to sustain normal keratin synthesis. Hair is essentially compressed, keratinized protein; when the building blocks are scarce, the body prioritizes other biological functions over hair growth. Both the metabolic stress of rapid weight loss and the nutritional gaps from reduced appetite act on the same hair follicle system simultaneously, which is why the effect in Zepbound patients can be more pronounced than in patients who lose weight more slowly.
Who Is Most at Risk for Hair Loss on Zepbound?
Not every patient on Zepbound loses noticeable amounts of hair. Several risk factors significantly increase individual susceptibility.
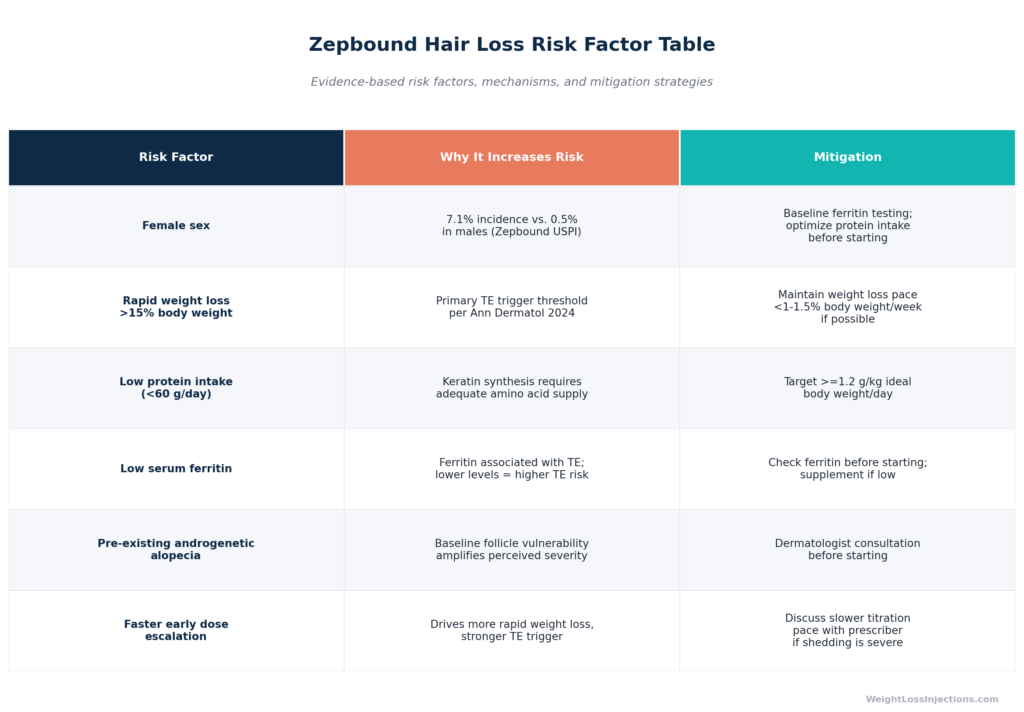
Zepbound hair loss risk factor table
Female Sex
The sex disparity in the Zepbound label data is striking and is consistent with broader dermatological literature. The 2024 Annals of Dermatology study (PMC) found that women are especially vulnerable to TE “even if the degree of weight loss is not more severe than in men and young adults.” In that study’s 140-patient cohort, 110 (78.6%) were women. The proposed explanations include hormonal cycling patterns (estrogen fluctuations during rapid body mass reduction), lower baseline ferritin reserves, and potentially hormonal responses to fat tissue redistribution. The bariatric surgery literature confirms the same pattern: a systematic review in Obesity Surgery (PMC) found that female sex was associated with OR 3.87 for post-surgical hair loss, though the confidence interval was wide.
Rate of Weight Loss
The Annals of Dermatology cohort study (PMC) established concrete thresholds: TE occurred at a mean weight loss percentage of ~15% and a mean rate of ~3.54 kg/month. Many Zepbound patients at 10–15 mg exceed this rate during the active escalation phase. Patients who lose weight faster, through higher doses, excellent adherence, or baseline metabolic characteristics, face a stronger TE trigger signal.
Iron Status and Ferritin
Iron deficiency is the most commonly identified nutritional precipitant of telogen effluvium. A 2021 study in Clinical, Cosmetic and Investigational Dermatology (PMC) found that serum ferritin levels were significantly lower in TE patients than in healthy controls, with the average ferritin in TE patients at 24.27 ng/mL. The study identified an optimal ferritin cut-off of 24.45 ng/mL for distinguishing TE patients from healthy subjects. A systematic review in Obesity Surgery (PMC) confirmed that low serum ferritin, along with low zinc and folic acid, was significantly associated with post-bariatric hair loss. Importantly, many women begin weight-loss treatment with borderline-low ferritin already: premenopausal women with high menstrual losses and inadequate dietary iron are at compounded risk once caloric intake decreases further.
Pre-existing Androgenetic Alopecia
Patients with baseline androgenetic alopecia (male or female pattern hair loss) already have a reduced density of follicles in active growth. When telogen effluvium overlaps with androgenetic alopecia, the perceived severity of shedding is substantially greater, even if the biological mechanism is the same. If you already notice thinning at baseline, discuss this explicitly with your prescriber before starting Zepbound.
Dose Escalation Pace
Faster titration to higher doses produces more rapid early weight loss, and therefore a stronger TE trigger. While the standard Zepbound titration schedule (increasing by 2.5 mg every ≥4 weeks) already represents the minimum interval, some patients escalate aggressively by adhering closely to the 4-week minimum at each step. From a hair perspective, maintaining a given dose for 6–8 weeks rather than 4 may reduce the rate of weight loss slightly, a tradeoff worth discussing with your prescriber if you are in a high-risk group (Zepbound prescribing information).
Timeline: When Does Hair Loss Start and How Long Does It Last?
This is the question that concerns patients most. The honest answer is that timing follows a predictable biological pattern, not an arbitrary schedule.
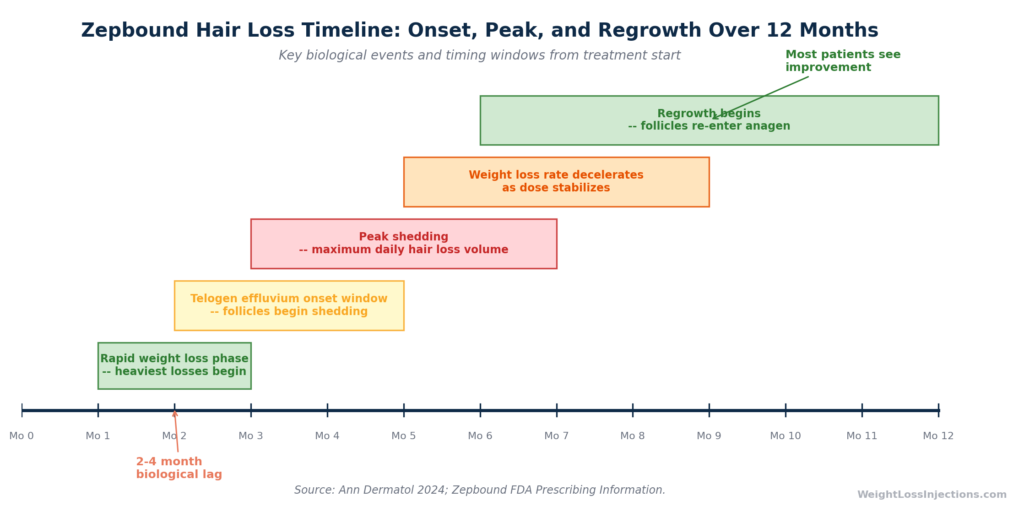
Zepbound hair loss timeline
Onset: 2–4 Months After the Trigger
The lag between physiological stressor and visible shedding is a defining feature of telogen effluvium, and one that consistently surprises patients. When rapid weight loss begins at months 1–2 of Zepbound therapy, the follicles that receive the stress signal spend the next ~3 months traversing the telogen phase before shedding. The result: patients often first notice significant shedding at months 3–5 of treatment, after they are already well into the drug and seeing positive results on the scale.
The Annals of Dermatology cohort (PMC) measured the mean duration between weight loss onset and hair loss onset at 1.12 months, reflecting variable timing across individuals. The commonly cited “2–4 months” represents the clinical range rather than a fixed threshold.
Peak Shedding: Approximately 1–3 Months After Onset
Shedding typically escalates for 1–3 months after it begins before plateauing. During peak shedding, patients may notice increased hair on pillows, in shower drains, and on brushes. Counting individual shed hairs obsessively is less useful than tracking whether visible density has decreased on scalp examination. Most patients experience diffuse thinning rather than concentrated patches, the diffuse pattern is characteristic of TE and distinct from the patchy loss of alopecia areata.
Resolution: 3–6 Months After Weight Loss Decelerates
The Annals of Dermatology study (PMC) found a mean recovery period of 4.83 months, and all patients in that cohort improved without any treatment. As Zepbound-treated patients reach maintenance doses and weight loss rate decelerates (typically months 5–9 of treatment), the physiological stressor diminishes. Follicles that have completed their telogen phase re-enter anagen, and regrowth begins, growing at approximately 0.5 inches per month. Most patients can expect meaningful regrowth between months 6 and 12 of treatment, with full density restoration often taking up to 12–18 months due to the slow pace of new hair emergence.
The key message: this is not permanent hair loss. No evidence from the Zepbound clinical trials or the broader weight-loss literature identifies telogen effluvium as causing scarring or permanent follicle damage. The Zepbound prescribing information notes that hair loss was associated with weight reduction, implying that the mechanism is the weight loss process, not irreversible drug toxicity.
Red Flags That Suggest a Different Diagnosis
Not all hair loss during Zepbound treatment is telogen effluvium. Contact your dermatologist if you experience any of the following, as these are not consistent with the telogen effluvium pattern:
- Hair loss beginning within the first 1–2 weeks of starting Zepbound (TE has a biological minimum lag; immediate loss suggests another cause)
- Patchy or asymmetric loss rather than diffuse thinning (consider alopecia areata)
- Scalp changes including redness, scaling, crusting, or scarring alopecia patterns
- Concurrent systemic symptoms such as fatigue, cold intolerance, constipation, or unexplained weight gain (consider thyroid evaluation — both hypo- and hyperthyroidism can cause hair loss independently)
- Hair loss that continues to worsen beyond 6 months without any plateau
- Loss of eyebrows, eyelashes, or body hair alongside scalp loss (suggests systemic or autoimmune causes)
How to Prevent and Minimize Hair Loss on Zepbound
Telogen effluvium cannot always be prevented, if you lose 15–20% of your body weight rapidly, some degree of TE is a likely biological outcome. But the severity can be modulated substantially through nutritional strategies and dose management.
Protein: The Most Critical Intervention
Hair is made primarily of keratin, a structural protein. Keratin synthesis requires a continuous supply of amino acids, particularly cysteine, methionine, and lysine, that are derived from dietary protein. When protein intake drops below minimum thresholds during caloric restriction, the body deprioritizes non-essential uses of amino acids (including hair growth) in favor of more critical functions.
Clinical nutrition guidelines for patients undergoing weight loss recommend a minimum of 1.2 g of protein per kg of ideal body weight per day, with a target of 1.5 g/kg/day preferred during the active weight loss phase. For a patient with an ideal body weight of 70 kg, that translates to 84–105 g of protein daily. Achieving this on a Zepbound-suppressed appetite requires deliberate planning:
- Prioritize protein first at every meal before eating other foods
- Choose protein-dense foods: chicken breast, Greek yogurt, eggs, cottage cheese, canned fish, tofu, legumes
- Consider a whey or plant-based protein supplement if food intake is very limited, protein shakes can contribute 25–30 g without significant volume
- Eat regular meals even when appetite is absent, skipping protein due to Zepbound-induced satiety accelerates both muscle loss and nutritional hair loss simultaneously
The evidence for protein’s role is not limited to Zepbound. The Obesity Surgery systematic review (PMC) found that low zinc, low folic acid, and low ferritin, all nutrients commonly depleted alongside protein during caloric restriction, were significantly associated with post-bariatric hair loss. A 2010 review in Bariatric Times noted 100% cessation of hair loss in patients supplemented with zinc in one study, underscoring that nutritional adequacy is a genuine modifiable risk factor.
Iron and Ferritin: Test Before You Start
Given the consistent evidence linking low ferritin to telogen effluvium, testing serum ferritin before beginning Zepbound, or early in treatment, is practical preventive medicine. The Clinical, Cosmetic and Investigational Dermatology study (PMC) identified a ferritin cut-off of ~24–30 ng/mL as associated with increased TE risk; while hair-specific optimal ferritin thresholds are debated (some dermatology sources cite 40–70 ng/mL as preferable for hair health), the practical clinical takeaway is that a ferritin below 30 ng/mL in a woman starting Zepbound warrants supplementation before weight loss begins. Iron supplementation requires provider guidance because excess iron has its own risks and absorption is affected by multiple factors.
Zinc, Biotin, and Vitamin D
These three micronutrients are commonly associated with hair health in patient-facing media, and they do play genuine roles in follicle function:
- Zinc is required for cell division in the hair matrix and has shown benefit in hair loss associated with zinc deficiency. The Bariatric Times review cited studies showing zinc supplementation reduced post-bariatric TE in zinc-deficient patients.
- Biotin (vitamin B7) is often marketed heavily for hair loss. Evidence supports biotin supplementation primarily in patients with documented biotin deficiency, which is rare in the general population. Routine high-dose biotin supplementation without confirmed deficiency is not evidence-based, and very high biotin doses can interfere with certain laboratory tests including thyroid panels.
- Vitamin D deficiency is associated with multiple forms of alopecia, including TE. Patients on caloric restriction who reduce dairy and fatty fish intake are at increased risk of deficiency. A standard vitamin D3 supplement (1,000–2,000 IU/day) is low-risk and commonly recommended during weight management.
The practical guidance: balanced, protein-prioritized eating that includes diverse whole foods will cover most micronutrient needs. Targeted supplementation of iron and possibly zinc is warranted if deficiency is confirmed or highly likely; blanket supplementation of biotin at megadoses is not recommended without confirmed deficiency.
Dose Pacing: A Conversation for Your Prescriber
If you develop significant hair shedding during dose escalation, your prescriber may consider maintaining your current dose for a longer interval, perhaps 6–8 weeks instead of the minimum 4, before advancing. This is not about stopping Zepbound; it is about moderating the rate of weight loss slightly to reduce the TE trigger signal. The Zepbound prescribing information specifies a minimum of 4 weeks between escalations but places no ceiling on how long a patient may remain at any given dose. Extending a maintenance period is a clinical option, not a treatment failure.
Do not stop Zepbound on your own to address hair loss. The weight regain following Zepbound discontinuation is substantial and rapid, SURMOUNT-4 (JAMA 2023) documented a mean weight regain of +14.0% over 52 weeks in patients who switched from tirzepatide to placebo after a period of successful weight loss. The disruption to your metabolic goals from stopping the medication is likely to far outweigh the temporary hair loss benefit.
Hair Care During Active Shedding
While dietary and pharmacological interventions address root causes, a few mechanical considerations can reduce unnecessary shedding:
- Use a wide-tooth comb or detangling brush on wet hair after applying conditioner; avoid aggressive brushing of dry tangled hair
- Minimize chemical treatments (perms, relaxers, bleaching) and heat styling during active shedding, these do not cause TE but can amplify breakage when hair is already fragile
- Consider low-level laser therapy (LLLT): evidence is limited for TE specifically, but devices cleared by the FDA for hair loss show an acceptable safety profile and may provide modest benefit in accelerating regrowth
- Volumizing shampoos and styling products can improve cosmetic appearance during the shedding phase without affecting the underlying biology
If Shedding Persists: Topical Minoxidil
If hair shedding continues beyond 6 months without plateauing, or if the density loss is severe and affecting your quality of life, topical minoxidil (2% or 5%) is a reasonable pharmacological option to discuss with a dermatologist. Minoxidil promotes follicle re-entry into the anagen phase by improving hair follicle blood flow via ATP-sensitive potassium channel activation and stimulating growth factor production from dermal papilla cells.
A 2025 open-label clinical trial published in The Journal of Dermatology (PMC) enrolled 12 subjects with TE (including cases triggered by crash diet) and applied 5% topical minoxidil twice daily for 24 weeks. Terminal hair count increased significantly by week 4, and at week 24, 80% of subjects were rated as “moderately improved” or better by investigators. Notably, all investigators and all subjects reported improvement at week 24. The authors noted that minoxidil application for TE remains off-label use and that the self-healing nature of TE complicates attribution, but concluded that the safety profile and wide availability support its use as a supportive therapy.
There is no known pharmacokinetic interaction between tirzepatide and topical minoxidil, but any new medication during Zepbound treatment should be reviewed with your prescribing provider.
When to See a Dermatologist
Most Zepbound-related hair loss does not require specialist evaluation, it is a predictable, self-limiting biological process. But dermatologist referral is appropriate in the following situations:
- Hair loss that does not fit the telogen effluvium pattern — patchy loss, scalp inflammation, eyebrow or eyelash involvement, or loss starting in the first weeks of treatment
- Shedding that continues to worsen beyond 6 months without any evidence of plateau or recovery
- Baseline androgenetic alopecia that you want to address proactively before starting Zepbound, combination therapy planning with minoxidil, finasteride, or other agents
- Psychological distress from hair loss — severe distress affecting quality of life warrants evaluation regardless of the expected clinical course; dermatologists can confirm diagnosis (via trichoscopy or scalp biopsy when necessary) and offer reassurance alongside treatment options
- Laboratory abnormalities such as markedly low ferritin, iron deficiency anemia, or abnormal thyroid function that may require specialist management beyond basic supplementation
A dermatologist can perform trichoscopy (scalp dermoscopy) to characterize the hair loss pattern accurately, distinguish TE from androgenetic alopecia or other causes, and confirm whether follicles retain regrowth potential.
Telehealth Support and Nutritional Monitoring
Preventing and managing hair loss on Zepbound is fundamentally a nutrition management challenge, and it is exactly the type of ongoing clinical problem that benefits from regular provider contact. Monitoring protein intake, checking ferritin and micronutrient levels, pacing dose escalation appropriately, and knowing when to refer to dermatology all require a provider who knows your case longitudinally, not a one-time telehealth visit.
Our take at WeightLossInjections.com: Hair loss is the Zepbound side effect that surprises patients most, because unlike nausea or fatigue, it does not announce itself during the first injection. It arrives months later, when patients are feeling great about their weight-loss progress, and it can be psychologically difficult even when the medical facts are reassuring. Our clinical position is this: the 7.1% incidence in women is high enough that every female patient starting Zepbound should be counseled about TE at their first visit — not in a way that causes alarm, but in a way that allows them to optimize protein intake proactively, test ferritin before weight loss begins, and recognize the symptom pattern if it emerges. Surprises are worse than prepared patients. A WeightLossInjections.com provider consultation includes nutritional planning as a standard component of Zepbound initiation — [$X/month] for bundled telehealth and ongoing monitoring ([service detail]).
Frequently Asked Questions
Does everyone on Zepbound lose hair?
No. Hair loss occurred in approximately 5% of pooled Zepbound clinical trial participants versus 1% on placebo per the Zepbound prescribing information. Among women specifically, the rate was 7.1%. While these are clinically meaningful numbers, the majority of patients, including the majority of women, do not experience noticeable hair loss. Risk is substantially higher in those who lose weight most rapidly, start with low ferritin, and eat inadequate protein. Proactive nutritional management reduces but does not eliminate the risk for those with multiple predisposing factors.
Is Zepbound hair loss permanent?
Based on the available evidence, no. Telogen effluvium, the mechanism behind Zepbound-related hair loss — is a reversible process. Follicles temporarily shift from the growth phase to the resting/shedding phase under metabolic stress, then cycle back to growth as the stress resolves. The Annals of Dermatology retrospective cohort (PMC) found that all 140 patients improved by an average of 4.83 months during follow-up without any treatment. The Zepbound prescribing information notes no patients discontinued treatment due to hair loss, consistent with the self-limiting nature of the condition. Permanent hair loss from Zepbound would require scarring alopecia, which is not a recognized feature of tirzepatide’s pharmacology.
When does hair loss start on Zepbound?
Most patients notice increased shedding approximately 2–4 months after the period of most rapid weight loss begins, which typically means months 3–5 of Zepbound treatment, though individual timing varies. This lag reflects the biological time required for telogen follicles to complete the resting phase before shedding. A smaller number of patients notice shedding earlier (months 2–3) or later (months 5–6). The Annals of Dermatology study (PMC) measured the mean onset at 1.12 months after weight loss began, though the range extended from 0 to 6 months.
What vitamins or supplements prevent hair loss on Zepbound?
No supplement prevents telogen effluvium if the primary trigger, rapid weight loss, remains active. However, ensuring nutritional adequacy meaningfully reduces severity. The highest-priority interventions are: (1) protein at ≥1.2 g/kg ideal body weight/day to maintain keratin synthesis; (2) iron/ferritin, test serum ferritin before starting, and supplement if below ~30 ng/mL, per Clinical, Cosmetic and Investigational Dermatology (PMC); (3) zinc, evidence from the bariatric hair loss literature suggests benefit in zinc-deficient patients; (4) vitamin D if intake from diet is reduced. High-dose biotin supplementation is widely marketed for hair but lacks strong evidence unless biotin deficiency is confirmed, and can interfere with laboratory tests.
Should I stop Zepbound if I’m losing hair?
No. Do not stop Zepbound without speaking to your prescriber. SURMOUNT-4 (JAMA 2023) demonstrated that stopping tirzepatide results in significant weight regain (mean +14.0% over 52 weeks), which undermines the clinical goals of treatment without meaningfully accelerating hair recovery, since hair loss resolves as weight stabilizes, not specifically when the drug stops. The more appropriate steps if shedding is severe are: discussing a longer hold at the current dose to slow weight loss rate, optimizing protein and micronutrient intake, and consulting a dermatologist to explore whether topical minoxidil is appropriate.
Why do women lose more hair on Zepbound than men?
The 14-fold sex disparity in the Zepbound label data (7.1% of women vs. 0.5% of men) reflects several biological differences. First, women are more vulnerable to TE in the weight-loss literature generally: the Annals of Dermatology study (PMC) found that women are susceptible to TE at lower weight-loss rates and percentages than men. Second, women on Zepbound also achieve greater absolute weight reductions across SURMOUNT trials, EurekAlert reporting on the sex-stratified SURMOUNT analysis (2024) found that female participants achieved weight reductions up to 24.6% versus 18.1% in males, reflecting the deeper TE trigger. Third, premenopausal women frequently have lower baseline ferritin reserves due to menstrual losses, and reduced dietary iron intake during caloric restriction can push ferritin below the threshold associated with TE risk. Fourth, hormonal changes accompanying rapid fat loss may affect the estrogen-follicle signaling axis in ways that are more pronounced in women. The interaction of all four factors likely explains the observed disparity.
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. Always consult your licensed healthcare provider before making any changes to your medication regimen.