
Zepbound Titration Timeline to Maximum 15 mg Dose
The FDA-approved maximum dose of Zepbound (tirzepatide) is 15 mg injected subcutaneously once weekly, for both the weight management and obstructive sleep apnea (OSA) indications. Getting there takes a minimum of 20 weeks through a structured titration schedule. At 15 mg, SURMOUNT-1 trial participants lost an average of 20.9% of body weight at 72 weeks, but most providers aim for the lowest effective maintenance dose, and the FDA label explicitly permits stepping back down if 15 mg is not tolerated.
The 15 mg Dose: What the FDA Label Says
The answer to the most common question on this topic is exactly one sentence from the Zepbound prescribing information, Section 2.2:
“The maximum dosage of ZEPBOUND for all indications is 15 mg injected subcutaneously once weekly.”
That sentence covers both FDA-approved uses of Zepbound: chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, and moderate-to-severe obstructive sleep apnea in adults with obesity. The FDA approved the weight management indication on November 8, 2023, and the OSA indication followed on December 20, 2024. In both cases, 15 mg is the ceiling, not a universal target.
There is an important distinction the Zepbound prescribing information draws between the two indications when it comes to the minimum maintenance dose. For weight management, the approved maintenance doses are 5 mg, 10 mg, or 15 mg weekly. For OSA, the approved maintenance doses are 10 mg or 15 mg weekly, the 5 mg dose is not approved for sleep apnea, reflecting the higher physiological response needed to meaningfully reduce apnea events.
The Approved Zepbound Dose Sequence
| Dose | Purpose | Pen Color | Notes |
|---|---|---|---|
| 2.5 mg | Tolerability start | Dark gray | Not a therapeutic dose |
| 5 mg | First maintenance option | Dark purple | Approved for weight management only |
| 7.5 mg | Titration step | Dark teal | — |
| 10 mg | Maintenance option | Pink | Approved for weight management and OSA |
| 12.5 mg | Titration step | Blue | — |
| 15 mg | Maximum dose | Red | Approved for weight management and OSA |
Source: Zepbound prescribing information; pen colors per Zepbound single-dose pen Instructions for Use.
How You Get There: The Titration Timeline
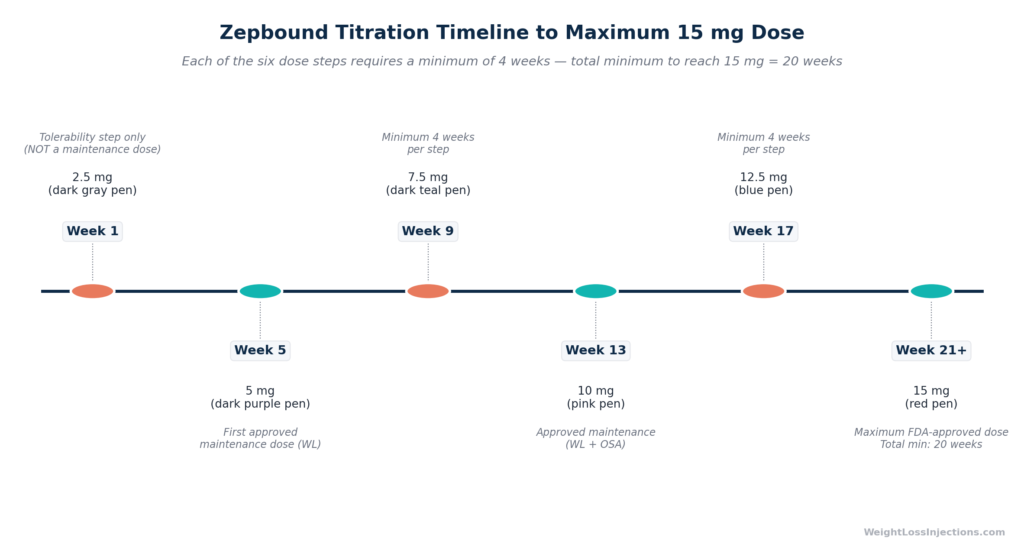
No one starts Zepbound at 15 mg. The FDA-approved titration schedule requires increasing the dose by 2.5 mg no more frequently than every four weeks. Starting from the 2.5 mg initiation dose, that produces the following minimum timeline:
- Weeks 1–4: 2.5 mg (tolerability step — not a therapeutic dose)
- Weeks 5–8: 5 mg
- Weeks 9–12: 7.5 mg
- Weeks 13–16: 10 mg
- Weeks 17–20: 12.5 mg
- Week 21 onward: 15 mg
The minimum time from first injection to 15 mg is therefore 20 weeks, or approximately five months. This is the fastest the label permits. In practice, many patients take considerably longer, six to twelve months is common, because tolerability holds at intermediate doses extend the timeline. A patient who experiences significant nausea at 7.5 mg may stay there for eight or twelve weeks before their provider determines it is appropriate to advance. The titration schedule is a floor, not a ceiling on time spent at each step.
The Zepbound prescribing information Section 2.1 gives prescribers explicit guidance on this point: “If patients do not tolerate a maintenance dosage, consider a lower maintenance dosage.” The label neither requires reaching 15 mg nor penalizes patients who stay at a lower effective dose.
What Does 15 mg Actually Achieve? Clinical Trial Data
Competitors who answer the “highest dose” question often stop at confirmation, yes, 15 mg is the max, here is the titration schedule, goodbye. That leaves patients without the most useful information: what does 15 mg actually do to body weight in a clinical trial, and how does it compare to lower doses?
The SURMOUNT program, five Phase 3 randomized trials of tirzepatide in adults with obesity or overweight, provides primary-source answers.
SURMOUNT-1: Non-Diabetic Obesity at 72 Weeks
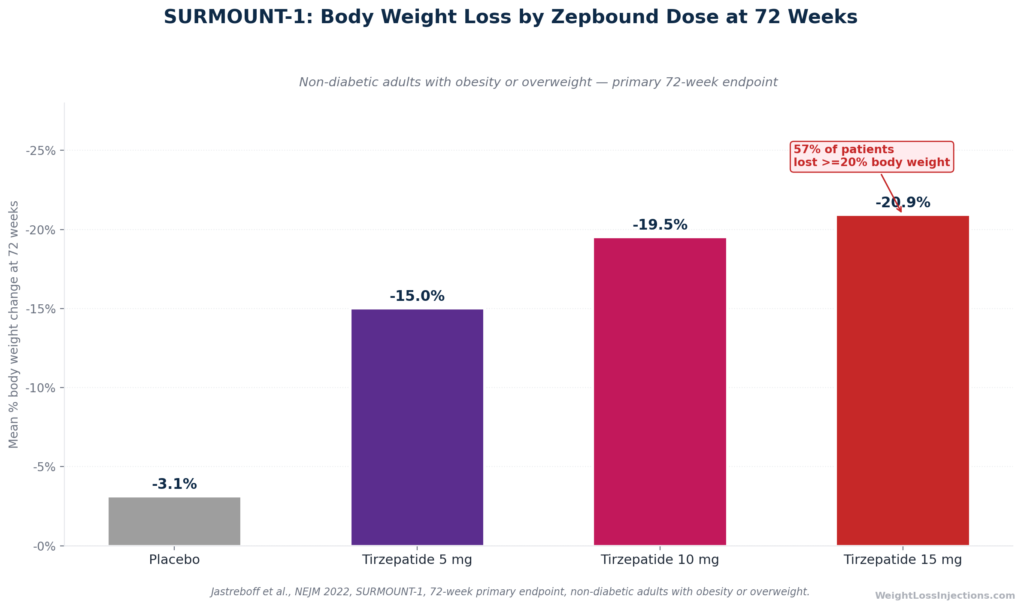
SURMOUNT-1 is the pivotal registration trial for Zepbound in adults without type 2 diabetes. Jastreboff et al., published in The New England Journal of Medicine (2022), enrolled 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one comorbidity over a 72-week primary treatment period.
Body weight results at 72 weeks (treatment-regimen estimand):
| Dose | Mean Weight Loss | ≥5% Weight Loss | ≥20% Weight Loss |
|---|---|---|---|
| Placebo | −3.1% | 35% | 3% |
| 5 mg | −15.0% | 85% | — |
| 10 mg | −19.5% | — | ~45% (estimated) |
| 15 mg | −20.9% | 91% | 57% |
Source: NEJM 2022, Jastreboff et al.; Lilly press release June 4, 2022.
A few things these numbers illustrate that competitors’ pages do not explain:
The 5-mg-to-15-mg efficacy gap is real but not dramatic. The jump from 5 mg (−15.0%) to 15 mg (−20.9%) at 72 weeks is about six percentage points of body weight, meaningful, but not a doubling of effect. Patients who are losing meaningful weight at 10 mg may not gain much by pushing to 15 mg, while taking on additional GI side-effect burden (discussed below).
The ≥20% body weight loss threshold is dose-dependent. At 15 mg, 57% of participants lost at least 20% of their body weight, an outcome that historically required bariatric surgery. That figure drops substantially at lower doses. For patients whose clinical goal requires very large weight loss, 15 mg is where the data supports pursuing that outcome.
Placebo-adjusted efficacy at 15 mg: −17.8 percentage points. Subtracting the placebo group’s 3.1% weight loss from the 20.9% achieved at 15 mg gives an estimate of the drug’s net pharmacological effect per ACC SURMOUNT-1 trial summary.
SURMOUNT-1 Body Weight Loss by Zepbound Dose at 72 Weeks
SURMOUNT-2: Obesity with Type 2 Diabetes at 72 Weeks
For patients with type 2 diabetes, SURMOUNT-2 tested only the two higher doses against placebo. Jastreboff et al., Lancet 2023 enrolled 938 adults with BMI ≥27 and T2D (HbA1c 7–10%). At 72 weeks, the 15 mg group achieved −14.7% mean body weight reduction (vs. −3.2% placebo), with 83% losing ≥5% body weight and a HbA1c reduction of −2.08%, per ACC SURMOUNT-2 summary. The lower weight loss compared to the non-diabetic population (−14.7% vs. −20.9%) is consistent across GLP-1 and dual agonist trials and reflects the metabolic differences of T2D patients, including insulin resistance and the weight-promoting effects of some concomitant diabetes medications.
SURMOUNT-4: Long-Term Maintenance at 88 Weeks
SURMOUNT-4 examined what happens when tirzepatide is continued at the maximum tolerated dose (10 or 15 mg) versus withdrawn. Published in JAMA 2023, participants who had already lost an average of −20.9% of body weight during a 36-week lead-in period were randomized to continue or stop. Continuers lost an additional 5.5% through week 88 (total −25.3%); those switched to placebo regained 14.0%. 89.5% of patients on continued tirzepatide maintained at least 80% of their lead-in weight loss at week 88, compared to just 16.6% on placebo. The core lesson: obesity requires long-term treatment, and stopping tirzepatide, at any dose, leads to substantial weight regain for most patients.
Side Effects at 15 mg Versus Lower Doses
The 15 mg dose is not simply “more of a good thing.” It carries a measurably higher gastrointestinal adverse event burden compared to lower maintenance doses, and this trade-off is exactly what the prescribing information describes when it instructs providers to weigh tolerability against clinical benefit.
GI Adverse Reactions: FDA Label Data
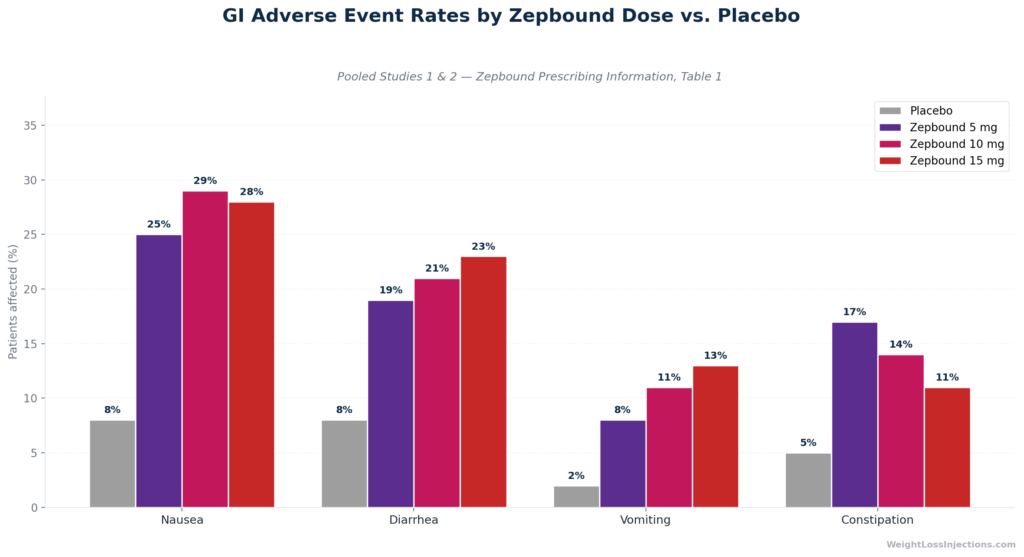
The following table is drawn directly from Table 1 of the Zepbound prescribing information, pooled from Studies 1 and 2 (SURMOUNT-1 and SURMOUNT-2):
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea† | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation‡ | 5% | 17% | 14% | 11% |
†Includes diarrhea and frequent bowel movements. ‡Includes constipation and feces hard.
Source: Zepbound prescribing information, Table 1.
A few patterns in the data that are not obvious from the summary numbers alone:
Nausea does not simply increase with dose. Nausea was actually slightly lower at 15 mg (28%) than at 10 mg (29%). This appears counterintuitive but reflects that patients titrating to higher doses have often developed more GI tolerance by the time they reach 15 mg, and that the pooled data combines long-term tolerators with early-treatment withdrawals at lower doses.
Diarrhea and vomiting do increase at 15 mg. Diarrhea (23% at 15 mg vs. 19% at 5 mg) and vomiting (13% vs. 8%) both show a dose-dependent increase. For patients who are sensitive to these effects, the incremental efficacy gain from 10 mg to 15 mg may not justify the additional GI burden.
Constipation runs opposite to the other GI effects. Constipation is highest at the 5 mg dose (17%) and actually decreases at higher doses (14% at 10 mg, 11% at 15 mg). This reflects two competing physiological mechanisms, the gastric-emptying slowing effect of GIP/GLP-1 agonism (which promotes constipation) is partially offset by the accelerated colonic motility that produces diarrhea at higher doses.
Severe GI adverse events increase with dose. The Zepbound prescribing information notes that severe GI adverse events occurred in 1.7% of patients at 5 mg, 2.5% at 10 mg, and 3.1% at 15 mg, compared to 1.0% on placebo. The overall GI adverse reaction rate across all Zepbound-treated patients was 56% versus 30% for placebo.
GI Adverse Event Rates by Zepbound Dose vs. Placebo
What to Do When GI Side Effects Are Severe
The GI side effects of tirzepatide are typically most pronounced during the first one to three weeks after each dose increase, not throughout the entire period at that dose. Most patients who experience nausea at a new dose find it manageable or resolved within two to four weeks as the body adapts.
The Zepbound prescribing information includes an important warning about dehydration: severe nausea, vomiting, and diarrhea can cause fluid loss significant enough to trigger acute kidney injury. Staying well hydrated, and contacting a provider if vomiting prevents normal fluid intake, is not optional safety advice, it is label guidance.
For patients experiencing severe or persistent GI adverse events at 15 mg, the prescribing information is explicit: “If patients do not tolerate a maintenance dosage, consider a lower maintenance dosage.” Reducing from 15 mg to 12.5 mg or 10 mg is an FDA-endorsed clinical option, not a treatment failure.
Who Should Reach 15 mg, and Who Shouldn’t
The goal of Zepbound titration is not to reach the highest possible dose. It is to find the lowest effective maintenance dose for each individual patient. The Zepbound prescribing information Section 2.1 states this directly: “Consider treatment response and tolerability when selecting maintenance dosage.”
Patients for Whom 15 mg May Be Appropriate
Patients who tolerate 12.5 mg without persistent or severe GI side effects. If the titration from 12.5 mg to 15 mg follows the minimum four-week schedule and does not produce intolerable adverse events, there is no label-based reason to stop short of 15 mg for a patient who has not yet achieved their clinical goal.
Patients with insufficient response at lower doses. A patient who has been at a stable 10 mg dose for several months and has not reached a meaningful weight-loss threshold, typically ≥5% body weight reduction, may benefit from dose escalation. The SURMOUNT-1 data shows a nearly five-percentage-point mean weight-loss difference between 10 mg (−19.5%) and 15 mg (−20.9%), which, while numerically modest at the mean level, can be clinically meaningful for individuals who are dose-limited rather than plateau-limited.
OSA patients who need further AHI reduction. Because the OSA indication requires a minimum maintenance dose of 10 mg (the 5 mg dose is not approved for OSA), OSA patients are already at higher doses than some weight-only patients. For patients whose apnea-hypopnea index reduction is insufficient at 10 mg, 15 mg is the logical next step per the FDA-approved OSA dosing.
Patients pursuing ≥20% body weight reduction. The SURMOUNT-1 data shows 57% of patients achieved ≥20% body weight loss at 15 mg, a threshold that many patients with severe obesity need to materially reduce comorbidities. For patients and providers targeting this level of response, 15 mg is the dose with the strongest evidence.
Patients Who May Be Well-Served at a Lower Dose
Patients achieving meaningful weight loss at 5 mg or 10 mg. Weight loss of ≥10% at 10 mg may be clinically sufficient for a given patient. Pushing to 15 mg adds GI burden for a marginal additional mean benefit at the population level.
Patients with persistent GI intolerance at 12.5 mg. Tolerability must be established before advancing. Escalating in a patient still experiencing significant nausea or diarrhea at 12.5 mg is not supported by the prescribing information.
Patients who have reached their target weight. SURMOUNT-4 showed effective weight maintenance on continued tirzepatide. A patient at goal weight on 10 mg has no evidence-based reason to escalate; 5 mg and 10 mg maintenance doses are not inferior for maintenance once weight loss goals are met.
15 mg for OSA: A Different Clinical Context
The OSA approval adds a layer of nuance to the dose question that most articles on this topic miss entirely. When Zepbound is prescribed for moderate-to-severe obstructive sleep apnea in adults with obesity, the approved maintenance doses are 10 mg or 15 mg only, the 5 mg option available for weight management is not on the OSA label per the Zepbound OSA dosing page.
The SURMOUNT-OSA trials — published in The New England Journal of Medicine, June 2024, enrolled 469 adults with moderate-to-severe OSA (AHI ≥15 events/hour) and obesity (BMI ≥30). At the maximum tolerated dose:
- AHI reduction: −25.3 events/hour in the non-PAP-therapy arm (vs. −5.3 events/hour placebo); −29.3 events/hour in the PAP-therapy arm
- OSA remission: 42% of tirzepatide patients in the non-PAP arm no longer had moderate-to-severe OSA at 52 weeks (vs. 16% placebo)
- Weight loss: Average approximately 18–20% body weight reduction
Source: Eli Lilly OSA approval press release; ACC SURMOUNT-OSA summary.
The minimum maintenance dose for OSA (10 mg) reflects the trial design: SURMOUNT-OSA used the maximum tolerated dose of 10 mg or 15 mg, not 5 mg. Patients prescribed Zepbound specifically for OSA should be aware that their minimum maintenance dose is higher than what weight-only patients may require, and that advancing to 15 mg, if tolerated, may produce further AHI reduction and weight loss.
Supply and Availability of 15 mg Zepbound
Shortage Status
As of April 2026, Zepbound is not in shortage. The FDA confirmed the tirzepatide shortage resolved on December 19, 2024, and all six dose strengths, including 15 mg, are available through standard pharmacy channels and LillyDirect. Earlier supply constraints that affected higher doses in 2023 and early 2024 are no longer a barrier to prescribing.
Compounding Status
Both 503A and 503B compounding windows for tirzepatide are closed as of early 2025, per FDA clarification. Only limited individualized exceptions remain for patients with documented allergies to branded excipients or unusual administration requirements. The 15 mg dose of Zepbound is available only as the FDA-approved branded product (Eli Lilly).
Device Options
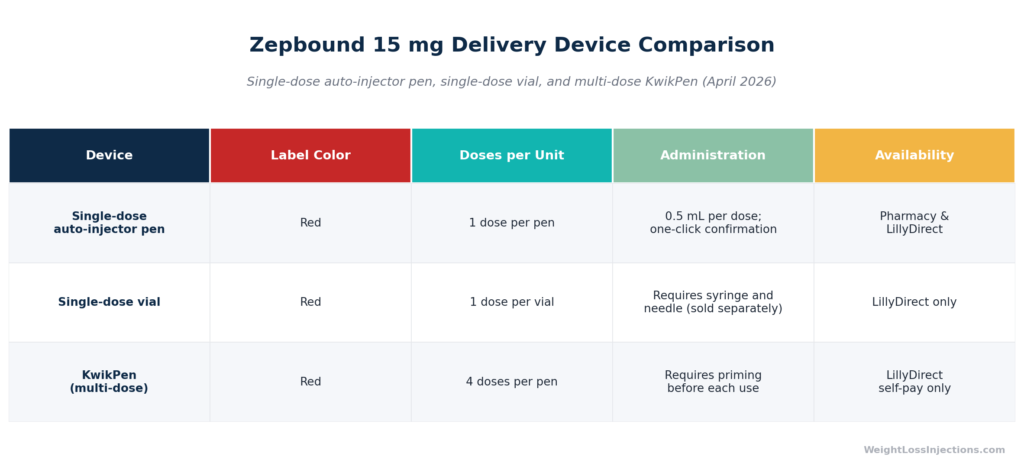
The 15 mg dose is available in all three current Zepbound delivery formats per Eli Lilly’s device lineup:
- Single-dose auto-injector pen (red label): One pen = one weekly dose. Available at all pharmacies carrying Zepbound and via LillyDirect.
- Single-dose vial: Draw with a separate syringe and needle. Available via LillyDirect for self-pay patients.
- Multi-dose KwikPen (launched February 23, 2026): Contains four doses per pen (one month of treatment). Available through LillyDirect for self-pay patients only; not yet available at traditional pharmacies as of April 2026. Source: CNBC Feb 23, 2026.
Zepbound 15 mg Delivery Device Comparison
Cost of the 15 mg Dose
One of the clearest advantages of Zepbound’s pricing structure is that the list price does not increase with dose strength. A 28-day supply at 15 mg costs the same as a 28-day supply at 2.5 mg.
Current Pricing as of April 2026
| Payment Path | 15 mg Monthly Cost |
|---|---|
| List price (WAC), all pharmacies | $1,086/mo |
| LillyDirect Self Pay Journey Program (vial or KwikPen) | $449/mo |
| Commercially insured with coverage (savings card) | As low as $25/mo |
| Commercially insured without coverage (savings card) | As low as $499/mo |
Sources: Eli Lilly pricing page; CNBC Dec 1, 2025; Zepbound savings program.
A few points worth noting:
LillyDirect flat pricing applies to all higher doses equally. Under the LillyDirect Self Pay Journey Program, all doses from 7.5 mg through 15 mg cost the same $449/mo — no price increase when titrating from 7.5 mg to 15 mg. Program enrollment and refill window adherence are required.
Medicare does not cover the weight management indication. Medicare Part D is statutorily prohibited from covering drugs prescribed solely for weight loss. As of April 2026, Zepbound for weight management is not covered under Medicare Part D, per the American College of Gastroenterology. A temporary Medicare GLP-1 Bridge program provides a $50 copayment option for eligible Part D enrollees from July 1 through December 31, 2026.
The OSA indication may unlock Medicare Part D coverage. Plans may cover Zepbound when prescribed for moderate-to-severe OSA, subject to formulary, per Wellcare Medicare guidance. Patients with both obesity and OSA should clarify which indication their prescription covers.
Safety Considerations Specific to the 15 mg Dose
Contraindications That Apply at Every Dose
The Zepbound prescribing information lists three absolute contraindications at any dose, including 15 mg: (1) personal or family history of medullary thyroid carcinoma (MTC), (2) Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), and (3) known serious hypersensitivity to tirzepatide or any Zepbound excipient. The black box warning applies uniformly: in rats, tirzepatide causes dose-dependent thyroid C-cell tumors at clinically relevant exposures. Human relevance is unknown. Patients should be counseled on thyroid tumor symptoms, neck mass, dysphagia, dyspnea, persistent hoarseness, and that routine calcitonin monitoring is of uncertain screening value.
Additional Precautions at Maximum Dose
The higher GI burden at 15 mg elevates the practical significance of several label warnings:
Dehydration and acute kidney injury. Diarrhea (23%) and vomiting (13%) at 15 mg can cause clinically significant fluid loss. The Zepbound prescribing information flags acute kidney injury as a risk when GI-mediated fluid losses are not replaced. Adequate hydration during the first weeks after reaching 15 mg is essential.
Hypoglycemia in patients on insulin or sulfonylureas. Glycemic suppression is greatest at the highest dose. Dose reduction of concomitant insulin or sulfonylurea should be considered, per the prescribing information.
Oral contraceptive interaction. Gastric emptying delay reduces oral drug absorption. Backup or alternative contraception is required for four weeks after the increase to 15 mg, per the prescribing information.
Anesthesia risk. Delayed gastric emptying creates aspiration risk during general anesthesia or deep sedation. Inform all providers of current Zepbound dose before any procedure.
Do not combine with Mounjaro or other GLP-1 agonists. Mounjaro and Zepbound both contain tirzepatide and must not be used together, per the FDA press release. The same applies to semaglutide, liraglutide, dulaglutide, and exenatide.
Our take at WeightLossInjections.com: The 15 mg dose of Zepbound is the highest approved because it is the highest dose studied in the pivotal trials — not because it is the universally correct destination for every patient. The SURMOUNT-1 data shows a real but modest efficacy increment between 10 mg and 15 mg (about 1.4 percentage points of additional mean weight loss). For patients who are tolerating lower doses well and meeting their clinical goals, pressing to 15 mg may offer marginal incremental benefit while introducing higher GI side-effect rates. Conversely, for patients who have plateaued, are managing severe obesity, or need the larger response to address a comorbidity like OSA, 15 mg is where the best published evidence lives. The decision belongs with a prescriber who knows your history, your tolerance profile, and your goals — not with a search result or a social media post. At WeightLossInjections.com, our licensed telehealth clinicians — including [DR. NAME, MD — PLACEHOLDER] — build individualized titration plans based on your response at each dose step, not a one-size-fits-all protocol. Our telehealth-managed Zepbound program starts at [$X/month], with [service detail]. If you’re wondering whether 15 mg is the right next step for you, that’s exactly the conversation to have with a clinician.
Frequently Asked Questions
What is the maximum dose of Zepbound?
The FDA-approved maximum dose of Zepbound for all indications, both weight management and obstructive sleep apnea, is 15 mg injected subcutaneously once weekly, per Zepbound prescribing information Section 2.2. No higher dose is approved, studied for long-term use, or available in any FDA-authorized format as of April 2026. The 15 mg dose is available as a single-dose auto-injector pen (red label), single-dose vial, and multi-dose KwikPen through LillyDirect.
How long does it take to reach the 15 mg dose?
At minimum, 20 weeks — progressing through five consecutive four-week steps (2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg) per the FDA-approved titration schedule. That is the fastest the label permits. In real-world prescribing, patients who need tolerability holds at intermediate doses, particularly 7.5 mg or 10 mg, where GI side effects are often most significant, typically take six to twelve months to reach 15 mg. Providers may also choose to pause titration if a patient is achieving good results at a lower dose.
Is 15 mg of Zepbound more effective than 10 mg?
Yes, modestly. In SURMOUNT-1 at 72 weeks, 15 mg produced −20.9% mean body weight loss versus −19.5% at 10 mg, a difference of approximately 1.4 percentage points, per Jastreboff et al., NEJM 2022. However, the proportion of patients achieving ≥20% body weight loss was higher at 15 mg (57%), which is clinically important for patients with severe obesity who need larger absolute weight reductions. The 15 mg dose also carries a higher rate of diarrhea (23% vs. 21%) and vomiting (13% vs. 11%) compared to 10 mg, per the Zepbound prescribing information. Whether the incremental efficacy justifies the incremental GI burden is an individual clinical decision.
What if I can’t tolerate 15 mg?
The Zepbound prescribing information Section 2.1 explicitly permits reducing to a lower maintenance dose: “If patients do not tolerate a maintenance dosage, consider a lower maintenance dosage.” Both 5 mg and 10 mg are FDA-approved maintenance doses for weight management with clinically meaningful efficacy demonstrated in SURMOUNT-1. Reducing from 15 mg to 12.5 mg or 10 mg is not a treatment failure, it is a recognized clinical pathway. Contact your prescriber before making any dose change; do not self-adjust.
Does the 15 mg dose cost more than lower doses?
No. The Zepbound list price (wholesale acquisition cost) of $1,086/mo applies uniformly to all six dose strengths for a 28-day supply, per Eli Lilly’s pricing. Under the LillyDirect Self Pay Journey Program, all doses from 7.5 mg through 15 mg are priced at $449/mo, the same price regardless of which dose in that range you are on, per CNBC Dec 1, 2025. For commercially insured patients with drug coverage, the Zepbound savings card can reduce the cost to as little as $25/mo.
Is 15 mg the maintenance dose for both weight loss and sleep apnea?
15 mg is an approved maintenance dose for both indications. However, the minimum maintenance dose differs. For weight management, the approved maintenance doses are 5 mg, 10 mg, or 15 mg once weekly. For OSA, the approved maintenance doses are 10 mg or 15 mg only, the 5 mg dose is not indicated for OSA per Zepbound OSA dosing information. OSA patients titrate through the same 2.5 mg → 5 mg → … → 15 mg sequence, but their minimum eligible maintenance dose is higher than that of weight-management-only patients.