
Ozempic Diarrhea Incidence by Dose vs. Placebo
Diarrhea affects approximately 8–9% of Ozempic users in clinical trials versus 1.9% on placebo, making it the third most common GI side effect after nausea and vomiting. It peaks during dose escalation (weeks 2–6) and typically resolves within 2–4 weeks as the body adjusts, but recurs with each dose increase. The serious concern is dehydration: the FDA has documented postmarketing cases of acute kidney injury, some requiring dialysis, in patients who experienced severe GI losses.
Manage diarrhea aggressively with fluids, dietary changes, and, when needed, OTC medications. Contact your provider if symptoms last more than 2–3 days without improvement, or if any red-flag signs appear.
Safety notice: This article is for educational purposes only. It does not constitute medical advice. If you are experiencing severe or persistent diarrhea on Ozempic, contact your prescribing provider promptly. Signs of dehydration or acute kidney injury require urgent medical evaluation.
What Is Ozempic Diarrhea?
Ozempic (semaglutide injection) is a GLP-1 receptor agonist approved by the FDA in December 2017 for glycemic control in adults with type 2 diabetes, with additional cardiovascular and chronic kidney disease indications added in subsequent years (FDA Ozempic Prescribing Information, 2025). Its most common adverse effects are gastrointestinal, and diarrhea is among the most frequently reported.
In clinical context, Ozempic-associated diarrhea presents as loose or watery stools occurring three or more times per day, often with urgency, and typically without the fever, blood, or severe cramping that would suggest an infectious etiology. It is physiologically distinct from infectious diarrhea: it arises from the drug’s direct and indirect effects on gut motility, nutrient absorption, and the enteric nervous system, not from a pathogen. Most episodes are mild to moderate in severity, self-limiting, and clustered in the dose-escalation window (FDA PI, 2025).
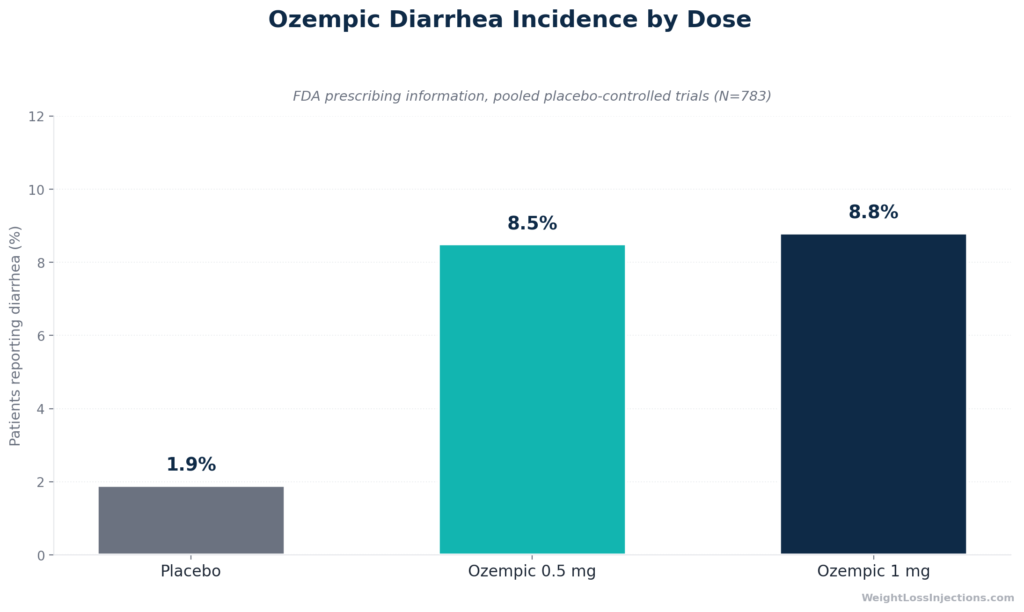
By frequency, diarrhea ranks as the third most common GI adverse event on Ozempic, after nausea and vomiting. In pooled placebo-controlled trials, 8.5–8.8% of patients experienced diarrhea on therapeutic doses, compared with 1.9% on placebo, giving a drug-attributable excess of roughly 6–7 percentage points (FDA PI, 2025). That sounds manageable in isolation, but the downstream risk, volume depletion leading to acute kidney injury, elevates this side effect from a nuisance to a safety concern that requires proactive management.
How Common Is Diarrhea on Ozempic?
Clinical Trial Incidence by Dose
The most reliable incidence data come from the FDA-reviewed pooled placebo-controlled trials submitted as part of Ozempic’s NDA (NDA 209637). The table below reproduces the exact figures from Table 1 of the FDA Ozempic Prescribing Information (2025):
| GI Adverse Reaction | Placebo (N=262) | Ozempic 0.5 mg (N=260) | Ozempic 1 mg (N=261) |
|---|---|---|---|
| Nausea | 6.1% | 15.8% | 20.3% |
| Vomiting | 2.3% | 5.0% | 9.2% |
| Diarrhea | 1.9% | 8.5% | 8.8% |
| Abdominal pain | 4.6% | 7.3% | 5.7% |
| Constipation | 1.5% | 5.0% | 3.1% |
Source: FDA Ozempic Prescribing Information, 2025 — pooled placebo-controlled trials.
Several observations are worth highlighting. First, the diarrhea rate jumps fourfold from placebo (1.9%) to Ozempic 0.5 mg (8.5%), the largest relative increase occurs at the first therapeutic dose, not at the higher dose. Second, the 0.5 mg and 1.0 mg rates are nearly identical (8.5% vs. 8.8%), suggesting a ceiling effect for diarrhea that does not parallel nausea, which increases substantially with dose. Third, overall GI adverse reactions affected 32.7% of patients at 0.5 mg and 36.4% at 1.0 mg versus 15.3% on placebo, confirming that diarrhea is one part of a broader GI burden (FDA PI, 2025).
These figures come from patients with type 2 diabetes in controlled trial settings. Real-world rates may differ based on concomitant medications, dietary patterns, and comorbidities. A 2024 meta-analysis in PubMed Central examining 12 randomized controlled trials (n=8,055) found that semaglutide was associated with significantly higher total GI adverse events compared with control groups (OR 3.40 vs. placebo, 95% CI 2.79–4.14, P<0.00001), consistent with the FDA PI figures and confirming that the GI signal is robust and reproducible across study populations (Huang et al., PMC 2024).
Discontinuation Rates
GI side effects are the primary reason patients stop Ozempic early. Per the FDA PI (2025), 3.1% of 0.5 mg patients and 3.8% of 1.0 mg patients discontinued treatment due to GI adverse reactions, compared with 0.4% on placebo. Diarrhea is a contributing factor but rarely the sole driver of discontinuation; nausea and vomiting account for the majority of GI-related stops.
Postmarketing Pharmacovigilance
Real-world adverse event data corroborate the trial signal. A 2024 analysis of the FDA Adverse Event Reporting System (FAERS) database, covering 19,289 semaglutide-related adverse drug event reports, found that gastrointestinal disorders were the single most commonly reported system organ class (SOC), accounting for 28.02% of all reported events (Zhang et al., Frontiers in Pharmacology, 2024). Within GI events, diarrhea was the third most frequently reported preferred term after nausea and vomiting, with 1,822 cases (3.25% of all PTs across both oral and subcutaneous formulations) (Zhang et al., Frontiers in Pharmacology, 2024). The same FAERS analysis identified a novel safety signal specifically for subcutaneous semaglutide: hemorrhagic diarrhea (reporting odds ratio 3.69, 95% CI 1.53–8.88), which had not been prominently flagged in pre-approval data (Zhang et al., Frontiers in Pharmacology, 2024).
Timing and Dose Relation
The pattern is consistent across all data sources: diarrhea is predominantly a dose-escalation phenomenon. Per the FDA PI (2025), “the majority of reports of nausea, vomiting, and/or diarrhea occurred during dose escalation.” In practical terms, this means symptoms typically appear within the first 1–2 weeks after starting a new dose or increasing to the next dose tier (usually weeks 2–6 of any given step). Most episodes last approximately 3 days, and prevalence declines as GI adaptation occurs over 2–4 weeks at a stable dose. When a patient escalates from 0.5 mg to 1.0 mg, or from 1.0 mg to 2.0 mg, the cycle can restart — though subsequent episodes are often milder than the first escalation.
Why Does Ozempic Cause Diarrhea?
The mechanism is multifactorial. No single pathway fully explains the diarrhea, but several well-supported mechanisms contribute.
Ozempic Diarrhea Mechanism Flowchart
Mechanism 1: Delayed Gastric Emptying and Altered Nutrient Absorption
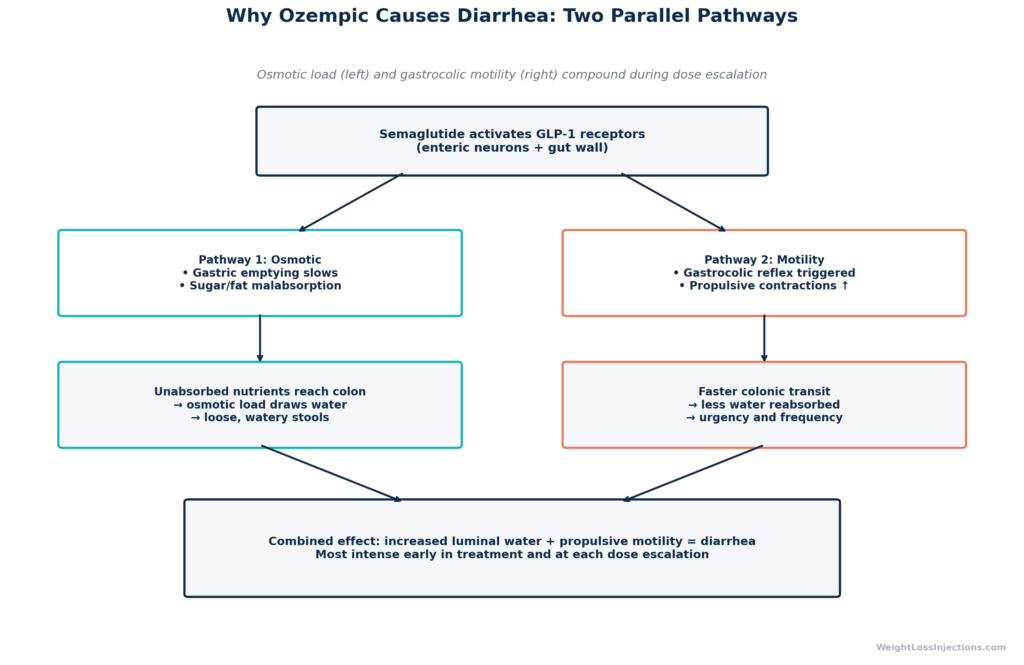
GLP-1 receptors are distributed throughout the enteric nervous system, including on neurons regulating gastric emptying and intestinal motility. Semaglutide activates these receptors pharmacologically, producing an initial deceleration of gastric emptying that slows the transit of food from the stomach into the small intestine (FDA PI, 2025). The paradox is that slowed gastric emptying does not uniformly slow everything downstream, it disrupts the coordinated timing of nutrient absorption.
When food moves through the small intestine at an altered rate, the usual synchronized absorption of simple carbohydrates and fats can be incomplete. Malabsorbed sugars and fats reach the colon, where they create an osmotic gradient that draws water into the bowel lumen, producing loose or watery stools. Simultaneously, GLP-1 receptor activation in the gut is thought to augment the gastrocolic reflex, the propulsive colonic contraction triggered by food entering the stomach, which can accelerate transit and increase stool frequency (Huang et al., PMC 2024). The net result, increased luminal water plus propulsive motility, is diarrhea.
The 2024 GI safety meta-analysis confirmed that GLP-1 receptors are widely distributed in enteric neurons and regulate GI motility, and that pharmacological activation by GLP-1 receptor agonists causes “rapid but incomplete desensitization,” meaning the GI effects diminish with sustained exposure but do not fully normalize at all doses (Huang et al., PMC 2024). This incomplete desensitization explains why diarrhea tends to recur with each dose increase even after tolerance has been established at the prior dose.
Mechanism 2: Overflow Diarrhea from Constipation
A counterintuitive but clinically important mechanism: constipation (which affects ~5% of patients at 0.5 mg per the FDA PI) can produce apparent diarrhea. When stool becomes impacted in the colon, liquid stool can leak around the obstruction and present as watery loose stools, a phenomenon known as overflow or paradoxical diarrhea (FDA PI, 2025). Patients experiencing both constipation and diarrhea on Ozempic, which is not uncommon, should be evaluated for this possibility before treating diarrhea with antidiarrheal agents, as loperamide would worsen an underlying fecal impaction.
Mechanism 3: Bile Acid Alterations
GLP-1 receptor activation affects upper GI motility in ways that alter bile acid transit and reabsorption. Normally, bile acids secreted into the duodenum are reabsorbed in the terminal ileum via active transport; altered transit timing can affect how much bile acid is reabsorbed versus passed to the colon. Bile acids reaching the colon stimulate fluid secretion and colonic motility, a well-characterized mechanism of bile acid diarrhea (Clinical and Translational Gastroenterology, PMC 2025). The extent to which this mechanism contributes to semaglutide-specific diarrhea (as opposed to other GLP-1 receptor agonists) is not fully established, but it is physiologically plausible and supported by the known relationship between GLP-1 receptor activation and intestinal bile acid handling (Journal of Clinical Endocrinology and Metabolism Case Reports, 2022).
Mechanism 4: Microbiome Shifts
Semaglutide alters gut microbial community composition, though the directionality and clinical significance of these shifts remain under active investigation. A 2024 study in the European Journal of Pharmacology found that semaglutide modulated gut microbiota composition in obese mice, including increases in Akkermansia muciniphila (associated with improved metabolic function) and changes in Lachnospiraceae and Bacteroides relative abundance (Duan et al., Eur J Pharmacol, 2024). A 2025 review of GLP-1 analogue effects on gut microbiota in Nutrients catalogued variable shifts across six preclinical semaglutide studies, with no consistent pattern emerging, and noted that no human microbiome studies had been completed at time of publication (PMC Nutrients review, 2025). Whether early microbiome disruption during semaglutide initiation contributes meaningfully to diarrhea in humans is biologically plausible but not yet established by clinical evidence. The clinically relevant point is that the gut is undergoing multiple simultaneous adjustments when semaglutide is introduced, and the GI side effect profile reflects that complexity.
How Long Does Ozempic Diarrhea Last?
Individual episodes are typically short. Data from Wegovy’s STEP 1–3 trial pool (semaglutide 2.4 mg, a higher dose with proportionally higher GI rates) show a median diarrhea episode duration of 3 days (Davies et al., Diabetes, Obesity & Metabolism, 2022). The Ozempic doses (0.5–1.0 mg) would be expected to show similar or shorter episode durations given lower drug exposure.
The broader arc matters more: diarrhea prevalence is highest during dose escalation and declines as the body adapts, typically over 2–4 weeks at any given dose level. Most patients who reach a stable maintenance dose and remain there see GI symptoms diminish substantially or resolve entirely. The important caveat is that dose escalation resets this clock. A patient who has been stable on 0.5 mg for three months may experience a new bout of diarrhea within the first 1–2 weeks of increasing to 1.0 mg, this is expected physiology, not treatment failure.
The 2024 meta-analysis found that long-term treatment (>30 weeks) was not associated with significantly higher overall GI adverse events compared with control (OR 1.38, 95% CI 0.85–2.21), consistent with progressive tolerance development over time (Huang et al., PMC 2024).
Summary timeline:
- Individual episode: median ~3 days
- Dose-escalation flare: typically peaks weeks 2–6 at any new dose
- Resolution at stable dose: usually within 2–4 weeks
- Recurrence risk: at each dose increase
Managing Ozempic Diarrhea at Home
Most diarrhea episodes on Ozempic can be managed without medical intervention, provided dehydration is prevented and no red-flag symptoms develop. The following strategies are evidence-informed and consistent with standard GI guidance.
Dietary Modifications
The foundational dietary intervention for acute diarrhea is the BRAT approach: Bananas, Rice, Applesauce, and Toast. These foods are low-fiber, low-fat, low-osmolarity, and easily absorbed — reducing the osmotic load in the gut. Patients on Ozempic experiencing diarrhea should temporarily avoid:
- Dairy products: Lactose can worsen osmotic diarrhea, particularly during GI distress when lactase expression may be transiently reduced.
- Fried and high-fat foods: Fat stimulates both bile acid secretion and the gastrocolic reflex; high-fat meals are particularly likely to trigger urgency.
- Caffeine and alcohol: Both accelerate colonic transit and can increase fluid losses.
- High-fiber foods: Insoluble fiber adds bulk and speeds transit; fiber supplementation that is appropriate during constipation can worsen diarrhea during acute episodes. Soluble fiber (oats, psyllium in small amounts) may be better tolerated.
- Sugar alcohols (sorbitol, xylitol, maltitol): Found in sugar-free gums, candy, and some protein bars; these osmotically active compounds directly worsen diarrhea.
Eating smaller, more frequent meals reduces the bolus load delivered to the intestine at any one time and blunts the gastrocolic reflex. Avoiding eating immediately before lying down may also reduce reflux-associated nausea that can compound GI discomfort.
Hydration and Electrolyte Replacement
Fluid replacement is the single most important management step and the primary defense against acute kidney injury (see Dehydration Risk section below). General fluid guidance for adults with mild to moderate diarrhea:
- 91–125 oz (approximately 2.7–3.7 liters) of total fluid per day, per standard Institute of Medicine hydration guidance for adults; losses from diarrhea increase this requirement further.
- Oral rehydration solutions (ORS) — commercially available as Pedialyte, Liquid I.V., LMNT, or WHO-formula ORS — are more effective than plain water for replacing sodium, potassium, and glucose-cotransported fluid. They exploit the sodium-glucose cotransporter in the gut, which remains functional even during diarrhea, driving fluid absorption.
- Avoid high-sugar beverages like sports drinks with ≥6% sugar (which can worsen osmotic diarrhea), apple juice, and caffeinated beverages.
Adequate hydration cannot be overemphasized. The FDA’s prescribing information explicitly instructs providers to “inform patients of the potential risk of acute kidney injury due to dehydration associated with gastrointestinal adverse reactions” and to “advise patients to take precautions to avoid fluid depletion” (FDA PI, 2025).
OTC Medications
Several over-the-counter options are available, with important caveats:
Loperamide (Imodium) is a synthetic opioid that reduces gut motility and increases anal sphincter tone. It is effective for controlling loose stools but should be used sparingly and not as a first-line default on Ozempic. The key caveat: if constipation is contributing to overflow diarrhea (see Mechanism 2 above), loperamide will worsen the underlying obstruction. Start with a 2 mg dose after the first loose stool; do not exceed 8 mg/day for self-treatment. Do not use if stools contain blood or if fever is present.
Bismuth subsalicylate (Pepto-Bismol, Kaopectate) has anti-secretory and mild antimicrobial properties. It can reduce stool frequency and volume without blocking motility, making it slightly safer than loperamide when the diarrhea mechanism is uncertain. Standard adult dose: 525 mg (2 tablets or 30 mL) every 30–60 minutes as needed, not to exceed 8 doses per day. Note: bismuth contains salicylate — avoid in patients with aspirin sensitivity or concurrent use of blood thinners.
Probiotics may help restore microbiome stability during treatment initiation and are generally safe. The best-supported strains for antibiotic-associated and medication-induced diarrhea are Lactobacillus rhamnosus GG and Bifidobacterium species. While no large RCT has specifically evaluated probiotics for semaglutide-associated diarrhea, the biological rationale and safety profile support their use as an adjunct. Timing: take at least 2 hours apart from any other medications.
Serious Risk: Dehydration and Acute Kidney Injury
This section warrants direct language. What begins as inconvenient diarrhea can escalate to a medical emergency.
The FDA has documented postmarketing cases of acute kidney injury (AKI) in patients treated with semaglutide — some of which required hemodialysis. The FDA PI states explicitly: “There have been postmarketing reports of acute kidney injury, in some cases requiring hemodialysis, in patients treated with semaglutide. The majority of the reported events occurred in patients who experienced gastrointestinal reactions leading to dehydration such as nausea, vomiting, or diarrhea” (FDA PI, 2025).
This is a postmarketing safety signal — not a theoretical risk. Volume depletion from GI losses reduces renal perfusion pressure; in patients with pre-existing kidney disease, reduced reserve, older age, concurrent use of diuretics or ACE inhibitors/ARBs, or NSAIDs, the threshold for AKI is lower. The FDA requires providers to “monitor renal function in patients reporting adverse reactions to OZEMPIC that could lead to volume depletion, especially during dosage initiation and escalation” (FDA PI, 2025). The official Ozempic website also lists “dehydration leading to kidney problems” under serious side effects with the instruction to “tell your health care provider right away” if nausea, vomiting, or diarrhea does not stop (Ozempic.com side effects page).
Red-Flag Dehydration Signs — Act Promptly
Contact your provider or seek urgent medical care if you develop any of the following:
- Dark yellow or amber-colored urine — indicates concentrated urine from volume depletion
- Significantly reduced urine output — fewer than three voids in 24 hours
- Dizziness or lightheadedness, especially on standing (orthostatic hypotension)
- Dry mouth, cracked lips, or sunken eyes
- Rapid heart rate at rest
- Inability to keep fluids down — if diarrhea is severe enough that you cannot replace fluid losses by drinking
Patients on concurrent diuretics, ACE inhibitors, ARBs, or NSAIDs face elevated risk and should notify their prescriber at the first sign of significant GI losses, without waiting for dehydration symptoms to develop.
When to Contact Your Doctor or Telehealth Provider
Home management is appropriate for mild, brief episodes. But diarrhea on Ozempic requires professional evaluation under the following conditions:
- No improvement after 2–3 days of dietary management and hydration
- Severe or incapacitating diarrhea — more than 6–8 watery stools per day
- Diarrhea accompanied by vomiting, which eliminates the ability to replace fluid losses orally
- Fever above 101°F (38.3°C) — suggests infectious etiology requiring separate evaluation
- Blood in stool — not expected from semaglutide; requires investigation for other causes
- Any signs of dehydration described in the section above
- Diarrhea that recurs with each dose increase and significantly impairs quality of life — this is a clinical signal to discuss dose titration modification or a longer hold at the current dose
Your prescriber has several options: extending the hold at the current dose (4–8 weeks instead of 4 weeks), reducing to the prior dose temporarily, or — in refractory cases — reassessing whether Ozempic is the appropriate drug for you. None of these decisions should be made unilaterally. Do not reduce or stop Ozempic without prescriber guidance; abrupt discontinuation does not require a taper but the clinical reason for stopping matters for your ongoing treatment plan.
WeightLossInjections.com offers telehealth consultations for exactly these situations — a licensed provider who can review your symptom timeline, assess your risk factors, and adjust your titration schedule accordingly. A telehealth visit is particularly well-suited to GI side effect management because it does not require labs or physical examination in most cases; the history and medication review are sufficient to guide a dose modification decision. Schedule a free consult to discuss your options at [$X/month] for [service detail].
Prevention: Reducing Diarrhea Risk Before It Starts
Several strategies reduce the incidence and severity of GI side effects during Ozempic initiation:
Adhere to the 0.25 mg initiation phase. The FDA-labeled starting dose of 0.25 mg for four weeks before escalating to 0.5 mg exists precisely to allow GI adaptation. Skipping or shortening this phase is the single most avoidable contributor to severe early GI events. This dose is not therapeutic — it is a ramp. Respecting it reduces the shock to the enteric nervous system (FDA PI, 2025).
Consider evening dosing. Some patients report that injecting in the evening means peak GI effects (which occur 24–48 hours post-injection for semaglutide) fall during hours when eating is minimal, reducing the interaction between GI slowing and food transit. This is not an FDA recommendation but is a widely used clinical practice. Consistency in injection timing matters.
Eat small, low-fat meals on injection day and the following day. The gastrocolic reflex and osmotic effects are amplified by large or high-fat meals. Smaller meals reduce the stimulus.
Avoid escalating to the next dose until your current dose is fully tolerated. The minimum is four weeks per the FDA label, but there is no ceiling on how long you can stay at a given dose. Patients who stay at 0.5 mg for eight or ten weeks before moving to 1.0 mg often report substantially fewer GI problems at escalation than those who advance on schedule.
Ozempic Diarrhea Compared to Other GLP-1 Medications
Diarrhea Rates: Ozempic vs. Wegovy vs. Mounjaro vs. Placebo
Wegovy (Semaglutide 2.4 mg)
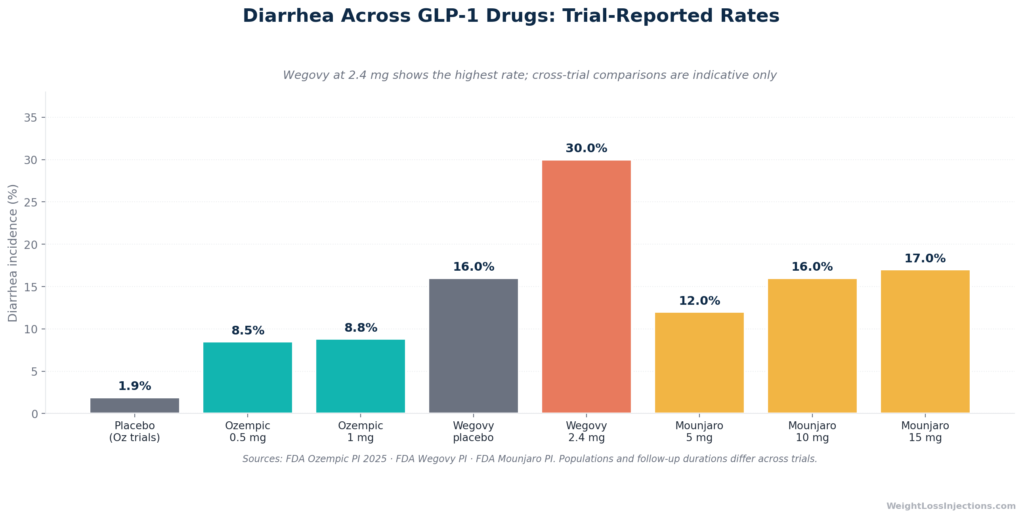
Wegovy is the same molecule as Ozempic, semaglutide. but at a higher maximum dose (2.4 mg weekly versus 1.0 mg for standard Ozempic glycemic dosing). The dose difference translates directly into higher GI side effect rates. Per the FDA Wegovy Prescribing Information (2026), diarrhea affected 30% of Wegovy-treated patients in pooled obesity trials versus 16% on placebo, a nearly 4-fold increase in drug-attributable risk compared with Ozempic’s 6–7 percentage point excess.
The STEP 1–3 trial GI tolerability analysis confirmed that 72.9% of Wegovy patients reported any GI adverse event versus 47.1% on placebo, with nausea (43.9%), diarrhea (29.7%), vomiting (24.5%), and constipation (24.2%) as the four most common (Davies et al., Diabetes, Obesity & Metabolism, 2022). Severe GI events (requiring medical attention or leading to treatment modification) occurred in 4.1% of Wegovy patients versus 0.9% on placebo (FDA Wegovy PI, 2026).
The important framing: Wegovy’s higher diarrhea rates are primarily a dose effect. Patients escalating to 2.4 mg are on a dose that is 2.4× higher than standard Ozempic glycemic dosing. The titration schedule for Wegovy is also longer (approximately 16 weeks to reach maintenance) precisely because the GI adaptation required is more substantial.
Mounjaro (Tirzepatide)
Mounjaro (tirzepatide) is a dual GIP/GLP-1 receptor agonist approved for type 2 diabetes management. Its GI profile differs from pure GLP-1 agents. Overall GI adverse events in pooled Mounjaro placebo-controlled trials affected 37.1–43.6% of patients at doses of 5–15 mg versus 20.4% on placebo (FDA Mounjaro Prescribing Information, 2025). Diarrhea is listed as one of the most common adverse reactions for Mounjaro, along with nausea, decreased appetite, vomiting, constipation, dyspepsia, and abdominal pain (FDA Mounjaro PI, 2025).
The Mounjaro label carries the same acute kidney injury / volume depletion warning language as Ozempic, reflecting the class-level mechanism: “Acute kidney injury has been reported in patients treated with MOUNJARO. The majority of the reported events occurred in patients who had experienced nausea, vomiting, diarrhea, or dehydration” (FDA Mounjaro PI, 2025).
Key comparison points:
| Drug | Active dose diarrhea rate | Placebo rate | AKI warning |
|---|---|---|---|
| Ozempic (semaglutide 0.5–1.0 mg) | 8.5–8.8% | 1.9% | Yes (postmarketing, some dialysis) |
| Wegovy (semaglutide 2.4 mg) | 30% | 16% | Yes |
| Mounjaro (tirzepatide 5–15 mg) | Part of overall GI 37–44% | 20.4% overall GI | Yes |
Sources: FDA Ozempic PI, 2025; FDA Wegovy PI, 2026; FDA Mounjaro PI, 2025.
The AKI / volume depletion warning is a class-wide concern — it appears in the labeling for all GLP-1 and dual GLP-1/GIP receptor agonists. The management principles (aggressive hydration, early provider contact) apply regardless of which agent you are taking.
Recent Studies and Postmarketing Data
Beyond the trial data, the postmarketing pharmacovigilance picture continues to develop.
The 2024 FAERS analysis by Zhang et al. in Frontiers in Pharmacology is among the most comprehensive pharmacovigilance analyses of semaglutide to date. Analyzing 19,289 semaglutide adverse event reports from the FAERS database (comparing oral versus subcutaneous administration), the authors found GI disorders were the dominant SOC for both routes — 30.19% of oral reports and 27.76% of subcutaneous reports. The analysis identified diarrhea (1,822 cases, 3.25% of PTs), constipation, and abdominal pain as the most consistently reported GI PTs after nausea and vomiting. Critically, the FAERS analysis identified a disproportionality signal for hemorrhagic diarrhea with subcutaneous semaglutide (ROR 3.69, 95% CI 1.53–8.88) — a rare but serious event not prominently featured in pre-approval trial data (Zhang et al., Frontiers in Pharmacology, 2024). This finding warrants attention: bloody diarrhea on semaglutide should always prompt urgent evaluation, as it may represent a serious GI event requiring investigation.
The 2024 GI safety meta-analysis from PubMed Central (12 RCTs, n=8,055) provides the most rigorous quantitative synthesis available. Key findings: semaglutide was associated with a 3.4-fold increase in GI adverse events versus placebo (OR 3.40, 95% CI 2.79–4.14); long-term treatment (>30 weeks) attenuated but did not eliminate the excess GI burden; and switching between GLP-1 agents or reducing dose did not reliably reduce GI adverse events — a counterintuitive finding with practical implications for patients seeking to manage GI side effects by switching drugs (Huang et al., PubMed Central, 2024).
Our take at WeightLossInjections.com: Diarrhea on Ozempic is common, predictable, and in most cases manageable — but it should never be dismissed. The combination of a medication that slows gastric emptying, alters nutrient absorption, and is taken long-term creates real dehydration risk, particularly during dose escalation. The FDA’s postmarketing warning about acute kidney injury, some cases requiring dialysis, is not a theoretical footnote; it is a documented safety outcome that patients and providers need to take seriously. Our practical recommendation: treat hydration as a non-negotiable daily priority throughout the titration phase, keep oral rehydration solution at home before you need it, and set a personal threshold for when you will contact your provider (our suggested threshold: any single day with more than 6 loose stools, or symptoms persisting more than 48 hours without clear improvement). The patients who manage Ozempic GI side effects best are the ones who have a plan before the side effects start — not the ones who improvise after two days of feeling miserable.
Frequently Asked Questions
Does Ozempic cause diarrhea?
Yes. Diarrhea is among the most common GI side effects of Ozempic, affecting 8.5% of patients on 0.5 mg and 8.8% on 1.0 mg in pooled placebo-controlled trials, compared with 1.9% on placebo (FDA Ozempic Prescribing Information, 2025). It is the third most common GI adverse event after nausea and vomiting. The majority of cases occur during dose escalation, not as a persistent steady-state effect.
How long does Ozempic diarrhea last?
Individual episodes typically last approximately 3 days, based on median duration data from semaglutide trials (Davies et al., Diabetes, Obesity & Metabolism, 2022). The period of heightened risk peaks during weeks 2–6 after starting or increasing a dose, then declines as GI adaptation occurs over 2–4 weeks. Diarrhea at a stable dose that has persisted beyond 4 weeks without improvement should prompt a provider evaluation.
What causes diarrhea on Ozempic?
Several mechanisms contribute: GLP-1 receptor activation slows gastric emptying and alters the absorption of sugars and fats, creating an osmotic load in the colon; it also augments the gastrocolic reflex, increasing colonic propulsion (Huang et al., PMC 2024). Altered bile acid transit through the small intestine may contribute additional secretory stimulus to the colon (Clinical and Translational Gastroenterology, PMC 2025). In some patients, apparent diarrhea is actually overflow from underlying Ozempic-related constipation (FDA PI, 2025).
Can Ozempic cause both diarrhea and constipation?
Yes — both are listed in the FDA prescribing information, and they can occur in the same patient at different times or alternate unpredictably. Constipation affects approximately 5% of patients at 0.5 mg and 3.1% at 1.0 mg (FDA PI, 2025). The GLP-1 mechanism affects the entire GI tract simultaneously but in ways that are not uniform — delayed gastric emptying can lead to constipation in the proximal gut while altered colonic motility produces urgency and loose stools. Some patients experience constipation as the dominant complaint initially, followed by loose stools as the body adjusts. Overflow diarrhea from hard stool impaction is a specific concern to rule out before treating loose stools with loperamide.
When should I see a doctor for Ozempic diarrhea?
Contact your provider if diarrhea: (1) has not improved after 2–3 days of dietary management and hydration; (2) is severe, more than 6–8 watery stools per day; (3) is accompanied by vomiting, fever, or blood in stool; (4) is causing signs of dehydration including dark urine, reduced urine output, or dizziness; or (5) recurs significantly with each dose increase and is affecting your quality of life or ability to take fluids (FDA PI, 2025; Ozempic.com). Telehealth consultation is appropriate for most of these situations and does not require an in-person visit.
Is Ozempic diarrhea dangerous?
Usually not, in isolation. Most cases are self-limiting and resolve within a few days. The danger arises from dehydration: the FDA has documented postmarketing cases of acute kidney injury, some requiring hemodialysis, in patients who experienced severe GI losses from semaglutide and became volume-depleted (FDA PI, 2025). Patients who are older, have underlying kidney disease, take diuretics or ACE inhibitors/ARBs, or are unable to maintain fluid intake during GI illness face elevated risk. Treat hydration as critical throughout the titration phase and respond promptly to any dehydration warning signs.
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. Always consult your licensed healthcare provider before making any changes to your medication regimen.