
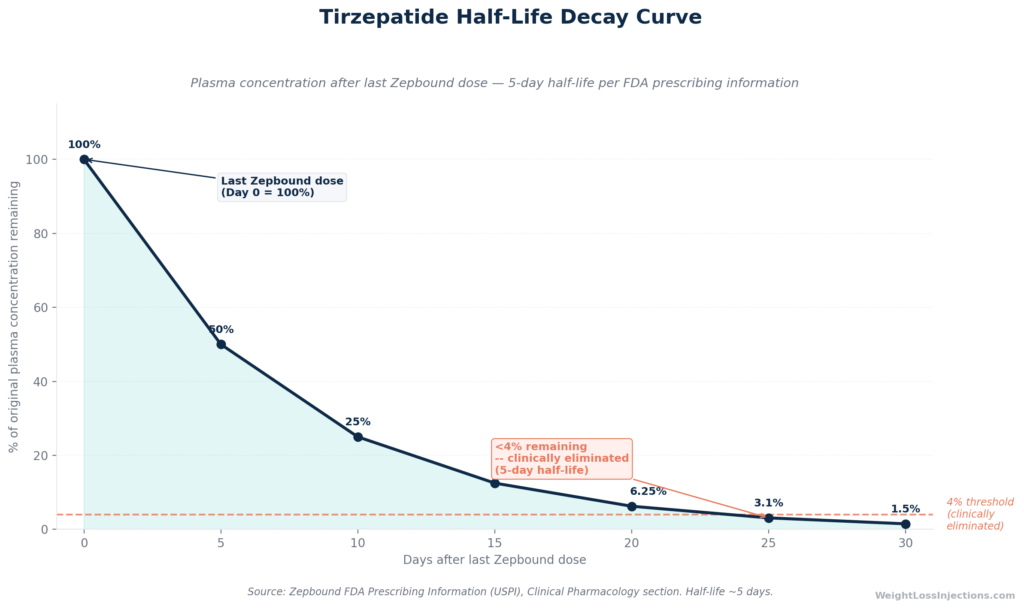
Zepbound (tirzepatide) has an elimination half-life of approximately 5 days, roughly half that of once-weekly semaglutide (Ozempic/Wegovy). After your last injection, it takes approximately 25–30 days, five half-lives, for tirzepatide to fall below 4% of its steady-state level, at which point it is pharmacologically negligible. Therapeutic effects like appetite suppression begin fading well before full clearance; most patients notice hunger returning within one to two weeks of stopping.
The drug’s elimination timeline is not meaningfully changed by kidney disease, liver disease, or body weight. And the clinical evidence from SURMOUNT-4 is unambiguous: patients who stop Zepbound regain the majority of their lost weight within a year without a transition plan.
What Is Zepbound and Why Does Its Half-Life Matter?
Zepbound is Eli Lilly’s brand name for tirzepatide injection, FDA-approved on November 8, 2023 for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity. A second indication, moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity, was approved on December 20, 2024, making Zepbound the only prescription drug approved for that indication.
Patients ask how long Zepbound stays in the body for at least five distinct reasons:
- Stopping or pausing treatment — Will weight regain start immediately? When will hunger return?
- Surgery — Will the drug’s gastric-emptying effects create aspiration risk during anesthesia?
- Pregnancy planning — When is it safe to conceive after stopping?
- Missing a dose — Has the drug significantly cleared before the next scheduled injection?
- Restarting after a gap — Is re-titration required, or can the previous dose be resumed?
This guide answers all five questions using the Zepbound FDA-approved prescribing information (USPI), the FDA clinical pharmacology review for NDA 217806, and the primary SURMOUNT trial publications. Competitors give a single-sentence answer, “about 30 days”, without explaining the mechanics, the variability, or the clinical implications. This article does all three.
Zepbound’s Half-Life: The Science Behind the 25–30 Day Timeline
What Is a Half-Life?
A half-life is the time it takes for the plasma concentration of a drug to fall by exactly 50%. Half-lives follow predictable first-order kinetics: after one half-life, 50% remains; after two, 25%; after three, 12.5%; and so on. The rule of thumb in clinical pharmacology is that five half-lives represent effective elimination, less than 3.1–4% of the original concentration remains, which is below the threshold of meaningful pharmacologic activity for most drugs.
Tirzepatide’s 5-Day Half-Life
Per section 12.3 of the Zepbound USPI, tirzepatide has an elimination half-life of approximately 5 days, or roughly 120 hours, following subcutaneous injection in patients with overweight or obesity. This is the half-life that enables once-weekly dosing. Some pharmacokinetic sources round to a range of 5–6 days (120–144 hours); the FDA pharmacology review for NDA 217806 documents this range across the SURMOUNT clinical population.
For comparison, semaglutide (Ozempic/Wegovy) has a half-life of approximately seven days, about 40% longer, which is why Ozempic requires five weeks to fully clear while Zepbound clears in roughly four to five weeks. The difference matters if you are planning surgery, switching medications, or timing a pregnancy.
Why Tirzepatide Lasts So Long in the Body
Native GLP-1, the incretin hormone that tirzepatide partially mimics, has a plasma half-life of approximately seven minutes before DPP-4 enzymes degrade it. Tirzepatide lasts 720 times longer. Two structural engineering choices explain this:
1. A C20 fatty diacid moiety at Lys-20. Per the FDA pharmacology review NDA 217806, a C20 fatty diacid (eicosanedioic acid) is attached via a γ-Glu–(AEEA)₂ linker at the lysine residue at position 20. This fatty acid anchor promotes tight binding to plasma albumin, which acts as a reservoir, bound drug is not filtered by the kidney and is protected from enzymatic degradation. Essentially the same strategy Novo Nordisk used for semaglutide’s C18 fatty acid chain, but applied to tirzepatide’s longer 39-amino-acid backbone.
2. Aib substitutions at positions 2 and 13. Alpha-aminoisobutyric acid (Aib) at these two positions introduces conformational rigidity that blocks DPP-4 cleavage, the primary enzymatic route for degrading GLP-1 family peptides, per the FDA pharmacology review NDA 217806. Without DPP-4 protection, tirzepatide would be broken down within hours.
The combined effect: a peptide that simultaneously binds two incretin receptors (GIP and GLP-1), making tirzepatide the first approved dual GIP/GLP-1 receptor agonist, while circulating in the bloodstream long enough to require only one weekly injection.
Half-Life Decay Table: What the Math Actually Looks Like
Using the 5-day half-life documented in the Zepbound USPI, the concentration decay after the last dose follows this progression:
| Day After Last Dose | Plasma Level Remaining | Clinical Interpretation |
|---|---|---|
| Day 0 (last dose) | 100% | Steady-state peak |
| Day 5 | ~50% | Appetite suppression still active |
| Day 10 | ~25% | Appetite beginning to return for most patients |
| Day 15 | ~12.5% | Sub-therapeutic for sustained weight loss |
| Day 20 | ~6.25% | Residual physiologic effect minimal |
| Day 25 | ~3.1% | Pharmacologically negligible |
| Day 30 | ~1.5% | Effectively eliminated |
After five half-lives, approximately 25 days, less than 4% of peak concentration remains. After 30 days, less than 2% remains. The Zepbound USPI confirms steady-state is achieved after approximately four weeks of once-weekly dosing, and clearance follows the same kinetic rate in reverse.
The practical bottom line: most clinical references to “30 days” for Zepbound clearance are conservative and accurate, they allow a modest safety margin above the pharmacokinetically calculated 25-day minimum.
Reaching Steady State: Why the First Month on Zepbound Matters
The same slow accumulation that makes Zepbound slow to clear also means it takes time to build up to therapeutic levels. Per the Zepbound USPI, steady-state plasma concentrations are achieved after approximately four weeks of once-weekly dosing.
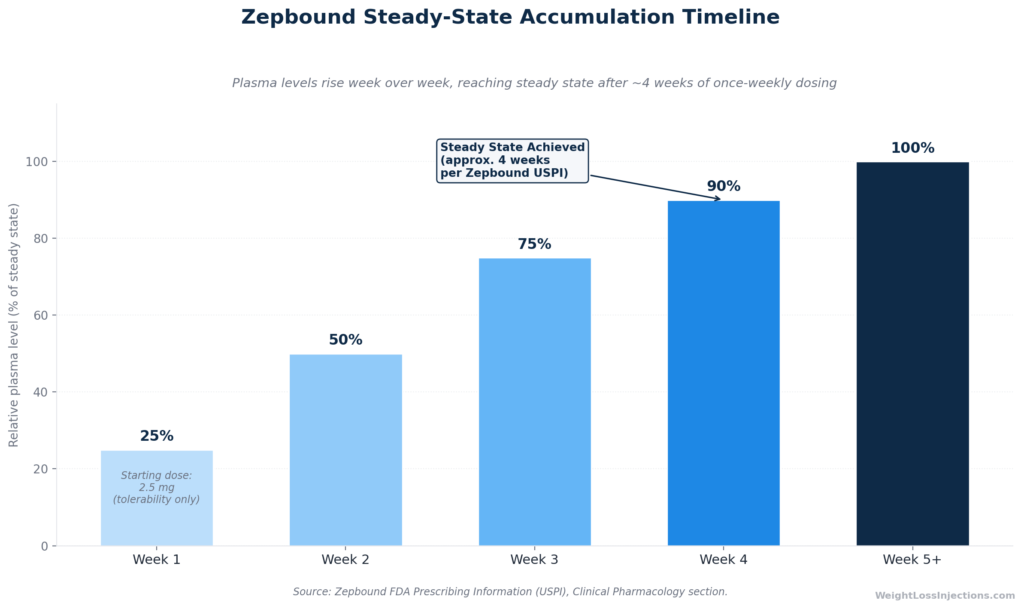
Zepbound Steady-State Accumulation Timeline
This has an important implication that most patients and even some providers underestimate: the 2.5 mg starting dose is a tolerability step only, it is not an approved maintenance or therapeutic dose, per the Zepbound USPI. The first four weeks of Zepbound treatment are a ramp-up phase during which drug levels are still building toward the therapeutic plateau. This is why patients often report modest appetite suppression in week one that strengthens noticeably by weeks three and four.
The Tmax: When Peak Concentration Occurs After Each Injection
After a subcutaneous injection, tirzepatide reaches peak plasma concentration (Tmax) in 8 to 72 hours, per the Zepbound USPI §12.3. The wide range, almost three days, reflects interindividual variability in subcutaneous absorption. Absorption speed can be affected by injection site (abdomen, thigh, and upper arm all have slightly different vascular density), injection technique, and individual differences in subcutaneous tissue. This Tmax range is meaningfully different from semaglutide’s 24–72 hours post-injection, tirzepatide can peak earlier, though the clinical significance for most patients is limited.
When Is Zepbound Fully Out of Your System?
The 25–30 Day Clearance Window
Based on the five-half-life principle and the 5-day half-life documented in the Zepbound USPI, tirzepatide is pharmacologically eliminated approximately 25 to 30 days after the last injection for the vast majority of patients. This is the answer most prescribers give and the range cited in reputable medical references.
The apparent discrepancy between some sources that say “25 days” and others that say “30 days” reflects the 5–6 day half-life range in the FDA pharmacology review: at exactly 5 days per half-life, five half-lives = 25 days; at 6 days per half-life, five half-lives = 30 days. Both figures are correct, they bracket the real-world clinical range. When planning surgery, pregnancy, or a medication switch, use the more conservative 30-day estimate.
Does Body Weight Change Clearance Time?
Body weight does not independently alter tirzepatide’s half-life in a clinically meaningful way. The Zepbound USPI states that no dose adjustment is required based on body weight, the pharmacokinetic profile is consistent across the patient population with overweight and obesity studied in SURMOUNT trials. A patient at 120 kg and a patient at 80 kg can both expect the same approximately 25–30 day clearance window.
Higher body weight does result in modestly lower absolute plasma concentrations at the same dose (due to larger volume of distribution), but this affects peak exposure level, not the half-life. A heavier patient starts from a slightly lower plateau, so the absolute amount remaining at day 25 is modestly lower, though the percent cleared is identical.
Does Kidney or Liver Disease Extend the Clearance Window?
No — not in a way that requires clinical adjustment. The Zepbound USPI explicitly states that no dose adjustment is required for patients with renal or hepatic impairment, because tirzepatide’s pharmacokinetics are not meaningfully altered by either condition.
This is mechanistically sensible. Tirzepatide is eliminated primarily through proteolytic degradation of the peptide backbone across multiple tissue compartments, not through renal filtration or hepatic CYP enzyme metabolism. The kidneys and liver are not the rate-limiting steps in tirzepatide clearance. Patients with chronic kidney disease or hepatic dysfunction can expect the same ~25–30 day washout as patients with normal organ function.
Does Dose Level Affect Clearance Time?
The half-life of tirzepatide does not change with dose, 2.5 mg and 15 mg have the same approximately 5-day half-life. What changes with higher doses is the absolute plasma concentration at steady state: a patient on 15 mg starts from a higher plateau than a patient on 2.5 mg. Both will reach pharmacologic elimination in ~25–30 days, but the higher-dose patient’s absolute plasma level at each time point is proportionally higher. The Zepbound USPI confirms linear, dose-proportional pharmacokinetics across the approved dose range.
What Happens to Your Body as Zepbound Clears
Appetite Suppression Fades Before Full Clearance
The appetite-suppressing effect of Zepbound, driven by GIP and GLP-1 receptor activation in the hypothalamus and brainstem, does not wait until Day 25 to fade. It begins tapering as plasma concentrations fall below the therapeutic threshold, which for most patients occurs somewhere in the 10–14 day range post-last-dose. This explains the common patient experience of “hunger returning in week two” after stopping.
This gradual taper mirrors the decay curve, not a cliff. Patients typically report:
- Days 1–7: Appetite suppression still largely intact; some mild increase in hunger
- Days 8–14: More pronounced return of hunger signals and “food noise”
- Days 14–25: Progressive return to baseline appetite; gastric emptying normalizing
- Day 25–30: Drug pharmacologically cleared; full baseline appetite restored for most
This is a behavioral and metabolic process, not a withdrawal syndrome. Tirzepatide does not produce physical dependence, per the Zepbound USPI.
Weight Regain: The SURMOUNT-4 Evidence
The most important clinical data on what happens after stopping Zepbound comes from SURMOUNT-4, published in JAMA in December 2023. This was a phase 3 randomized withdrawal study: 783 participants spent 36 weeks on tirzepatide (achieving a mean weight loss of 20.9%), then 670 were randomized 1:1 to either continue tirzepatide or switch to placebo for an additional 52 weeks.
The results were stark:
| Group | Weight change (weeks 36–88) | Overall change (weeks 0–88) |
|---|---|---|
| Continued tirzepatide | −5.5% (additional loss) | −25.3% total |
| Switched to placebo | +14.0% (regain) | −9.9% total |
Per SURMOUNT-4 (JAMA 2023) and the PubMed abstract, the estimated treatment difference between the two groups was −19.4 percentage points at week 88. Only 16.6% of patients who stopped tirzepatide maintained ≥80% of their lead-in weight loss at week 88, versus 89.5% of those who continued.
The key lesson: Weight regain begins well before the drug is fully cleared. The mechanism is behavioral — as GIP/GLP-1 receptor activation wanes, hunger increases and food intake rises, initiating regain before Day 25. Stopping Zepbound without a transition plan (behavioral support, dietary adjustment, or a stepdown strategy) leaves patients pharmacologically unprotected against the appetite drive that obesity generates chronically.
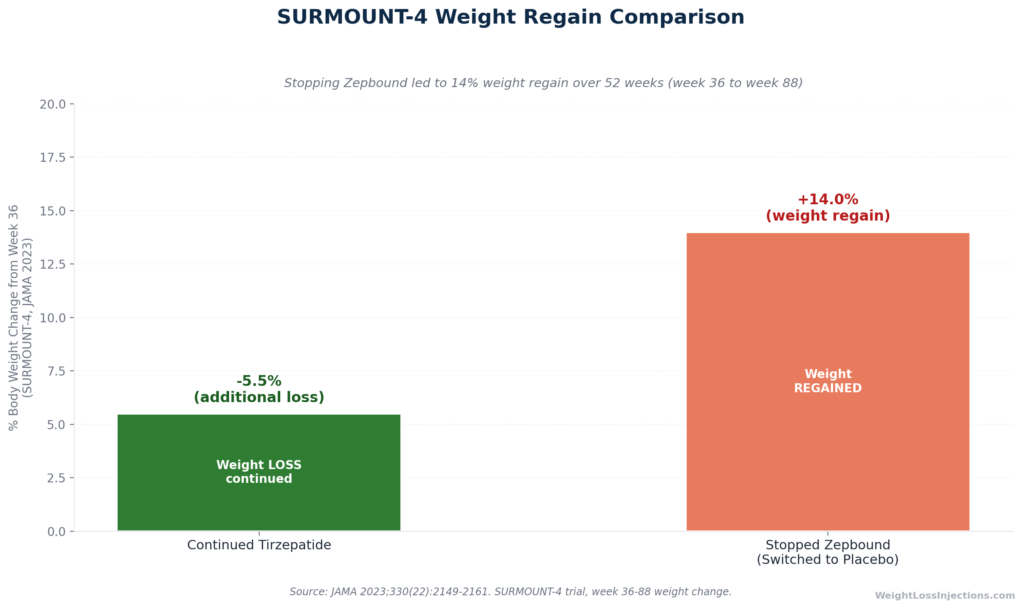
SURMOUNT-4 Weight Regain Comparison
Four Practical Scenarios: What the Clearance Timeline Means for You
Scenario 1: You Missed a Dose
Because tirzepatide’s 5-day half-life means approximately half the drug clears every five days, a single missed injection does not rapidly strip the drug from your system. The Zepbound USPI provides specific missed-dose guidance:
- If ≤4 days (96 hours) have passed since the missed dose: inject as soon as possible, then resume your normal weekly schedule.
- If >4 days have passed: skip the missed dose entirely and resume on your next regularly scheduled day. Do not take two doses within 3 days of each other.
The pharmacokinetic rationale: at 4 days post-missed-dose, approximately 57% of that week’s dose is still present (less than one half-life elapsed). Beyond 4 days, the plasma level has dropped enough that recovering the dose provides diminishing benefit and double-dosing creates GI side-effect risk.
Scenario 2: You Are Having Surgery or a Procedure
Tirzepatide slows gastric emptying as part of its mechanism, this is why patients feel full longer and eat less. But delayed gastric emptying persists for as long as the drug is pharmacologically active, meaning it can persist for up to 30 days post-last-dose as concentrations taper.
The anesthesia safety concern: patients with delayed gastric emptying may have food or liquid in their stomach even after standard pre-operative fasting, creating aspiration risk during general anesthesia or deep sedation. The Zepbound USPI’s Warnings and Precautions section specifically identifies this: “Inform patients about the risk of aspiration if they undergo procedures requiring general anesthesia or deep sedation while on treatment.”
Clinical guidance from anesthesiology societies has evolved rapidly on this topic. Many surgical centers now require patients to hold GLP-1/GIP agonists for 1–4 weeks prior to elective procedures requiring general anesthesia, though specific protocols vary by institution. The standard recommendation from the American Society of Anesthesiologists is to hold weekly GLP-1 agonists for one week before elective surgery; some centers apply a longer hold. Given Zepbound’s 25–30 day full clearance window, patients planning elective surgery should inform their surgical team at least 4–6 weeks in advance to allow adequate time for any required hold.
Scenario 3: Restarting After a Gap of More Than Two Weeks
When patients stop Zepbound and then wish to resume, the key question is: does the drug’s tolerance carry over? The answer depends on the length of the gap. If the gap exceeds two weeks (approximately 14 days), tirzepatide levels have fallen substantially, to roughly 25% or less of peak concentration. At this lower level, re-exposure at the prior maintenance dose can reproduce the GI side effects (nausea, vomiting, diarrhea) that the initial slow titration was designed to minimize.
The Zepbound USPI does not specify a formal re-titration requirement based on gap duration, but most prescribers apply the clinical judgment that a gap of more than two weeks warrants a provider consultation before resuming at the same dose. Your WeightLossInjections.com provider can assess whether dropping back a dose level for 4 weeks is prudent, or whether resuming at the prior dose is appropriate given your individual history.
Scenario 4: Stopping for Pregnancy
Zepbound may cause fetal harm. The Zepbound USPI §8.1 states that animal reproductive studies showed fetal growth reductions and malformations at clinically relevant exposures in rats and rabbits, and advises patients to discontinue when pregnancy is recognized. A pregnancy exposure registry exists at 1-800-LillyRx.
Unlike semaglutide, which the FDA label requires stopping at least two months before a planned pregnancy, the Zepbound USPI does not specify a minimum pre-conception washout period by number of weeks. Given the shorter 5-day half-life (vs. semaglutide’s ~7 days) and 25–30 day full clearance, most reproductive medicine providers recommend a 4–6 week buffer after the last injection before attempting conception. However, because reproductive timing is individual and involves factors beyond drug clearance, any patient considering pregnancy while on Zepbound should discuss the exact stop date with both their Zepbound prescriber and their OB-GYN or reproductive endocrinologist well in advance.
Drug Interactions: What Can Affect Tirzepatide’s Action
Oral Contraceptives
Tirzepatide’s gastric-emptying delay reduces the absorption rate of orally administered medications taken concurrently. The most clinically significant example involves oral contraceptives. Per the Zepbound USPI, patients using oral contraceptive pills should use backup or alternative contraception for 4 weeks after starting Zepbound and for 4 weeks after each dose increase. Gastric emptying normalizes after this period, at which point oral contraceptive absorption returns to baseline.
This interaction does not affect the clearance of tirzepatide, it affects the absorption of the co-administered oral drug. But it is relevant context for patients managing reproductive health while on Zepbound.
Other GLP-1 or GIP/GLP-1 Agonists
Zepbound must not be combined with other GLP-1 receptor agonists (semaglutide, liraglutide, dulaglutide, exenatide) or with Mounjaro, the same tirzepatide molecule in its FDA-approved T2D formulation. Per the FDA press release for Zepbound approval, concurrent use of any two tirzepatide-containing products, or of tirzepatide with another GLP-1 agonist, is contraindicated due to additive GI side-effect risk and potential for excessive pharmacologic effect.
When switching from semaglutide to tirzepatide, there is no mandatory washout, the drugs work through the same receptor pathway, so overlap creates additive but not dangerous effects for most patients. In practice, most providers time the first tirzepatide injection to coincide with the date the next semaglutide injection would have been due, minimizing the gap while avoiding actual overlap.
Insulin and Sulfonylureas
The Zepbound USPI flags hypoglycemia risk when tirzepatide is combined with insulin or sulfonylureas (not a typical scenario for the weight management indication, but relevant for patients who also have type 2 diabetes). Dose reduction of concomitant insulin or sulfonylurea may be required. As tirzepatide clears over the 25–30 day post-stop window, this hypoglycemia risk diminishes, but blood glucose should be monitored through the clearance period in any patient on insulin or a sulfonylurea.
Factors That Influence Your Individual Clearance: A Summary
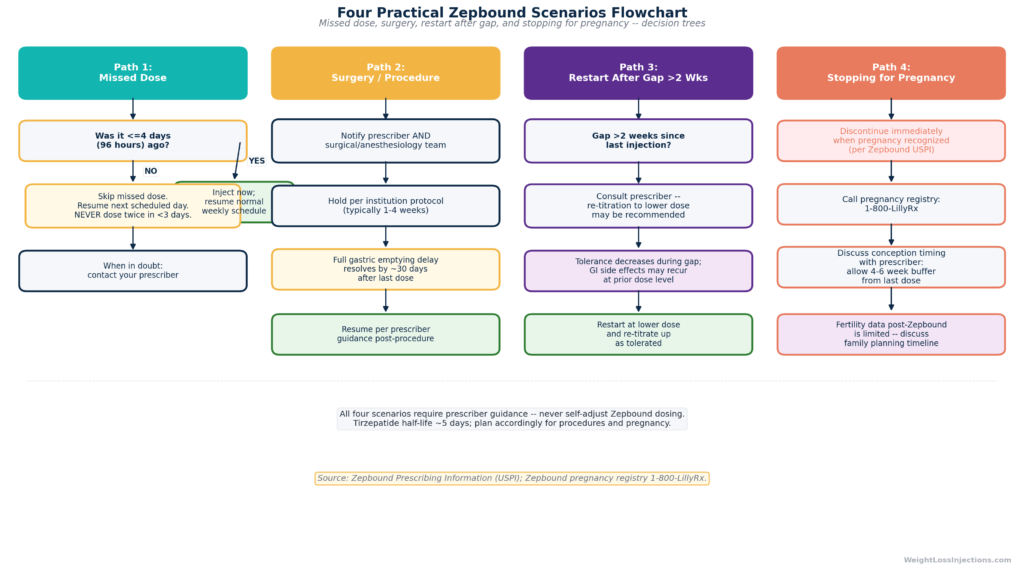
Four Practical Scenarios Flowchart
| Factor | Effect on Tirzepatide Clearance |
|---|---|
| Renal impairment | No clinically significant change — no dose adjustment required per Zepbound USPI |
| Hepatic impairment | No clinically significant change — no dose adjustment required per Zepbound USPI |
| Dose level | Same half-life at all doses; higher doses mean higher absolute plasma levels but identical % decay rate |
| Body weight | Minor effect on volume of distribution; no dose adjustment required; half-life essentially unchanged |
| Age | Not independently validated as altering tirzepatide half-life in the SURMOUNT population |
| Injection site | Affects Tmax (8–72 hours) but not half-life or total clearance time |
| Sex | Not a documented independent modifier of tirzepatide half-life per Zepbound USPI §12.3 |
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: The 25–30 day clearance window for Zepbound is one of the most clinically consequential pharmacokinetic facts your prescriber should discuss with you at the start of treatment, but in practice, it rarely comes up until a patient is planning surgery, trying to get pregnant, or already noticing weight regain after stopping. Understanding the decay curve in advance changes the decisions you make.
If you are stopping Zepbound intentionally, whether for pregnancy, a planned procedure, or personal preference, the SURMOUNT-4 data deserve serious attention: a +14.0% weight regain in the placebo group within 52 weeks is not a worst-case scenario, it is the median outcome, per JAMA 2023. That is not a criticism of the drug; it reflects the chronic biology of obesity. Stopping tirzepatide removes pharmacologic appetite control from a system that obesity has dysregulated. The 25-day window during which the drug clears is the window in which a behavioral and dietary transition plan needs to be in place.
At WeightLossInjections.com, our telehealth providers can help you map out that transition, whether you are planning to stop, restart, or simply want to understand what to expect at each point in the dosing cycle. Bundled telehealth and medication management starts at [$X/month] for [service detail]. Take our free eligibility quiz to be matched with a licensed prescriber in your state.
Frequently Asked Questions
How long does it take for Zepbound to fully leave your body?
After your last Zepbound injection, tirzepatide takes approximately 25 to 30 days to be pharmacologically eliminated, based on a half-life of approximately 5 days per the Zepbound FDA prescribing information. At 25 days (five half-lives), less than 4% of the peak steady-state concentration remains, a level considered clinically negligible. At 30 days, less than 2% remains. The reason some sources say 25 days and others say 30 days is the documented half-life range of 5–6 days in the FDA pharmacology review for NDA 217806: at the short end (5 days × 5 half-lives = 25 days) and at the long end (6 days × 5 half-lives = 30 days). For planning purposes, use 30 days as the conservative estimate.
How long until Zepbound’s effects wear off after stopping?
The pharmacologic effects of Zepbound begin fading before the drug is fully cleared. Appetite suppression starts diminishing approximately one to two weeks after the last injection as plasma concentrations drop below the therapeutic threshold. Gastric emptying delay, which affects both the sensation of fullness and the aspiration risk relevant to anesthesia, also tapers over this same window, with most effects resolved by the full 25–30 day clearance window. The return of appetite is gradual, not abrupt, because the decay follows first-order kinetics (a smooth curve, not a cliff). Per the SURMOUNT-4 withdrawal data published in JAMA 2023, measurable weight regain begins within weeks of stopping, well before Day 25, because hunger increases as drug levels fall.
Do I need to retitrate Zepbound if I miss more than 2 weeks?
There is no explicit re-titration protocol for a gap of more than two weeks in the Zepbound USPI, but the practical pharmacokinetic rationale is clear: after 14 days, roughly 25% of the prior dose level remains, meaning GI tolerance established during the original titration has substantially decreased. Most prescribers recommend consulting your provider before resuming if your gap exceeds two weeks, as resuming at the full prior maintenance dose may reproduce the nausea, vomiting, or diarrhea you experienced during initial titration. Dropping back one dose tier and re-titrating over 4 weeks is a common clinical approach, though the decision should be individualized. If your gap is less than two weeks (14 days), discuss with your prescriber, but re-titration is generally less likely to be required.
Can I have surgery while Zepbound is still in my system?
You should inform your anesthesiology team if Zepbound is or recently has been in your system. The drug’s gastric-emptying delay persists for as long as plasma concentrations remain pharmacologically significant, potentially up to 30 days after the last injection, creating aspiration risk during general anesthesia or deep sedation. Per the Zepbound USPI Warnings and Precautions, patients should inform all healthcare providers before any procedure requiring anesthesia. Most surgical centers now require a 1–4 week pre-operative hold for GLP-1/GIP agonists, though protocols vary. For elective procedures, plan your last Zepbound injection at least 4 weeks before your surgery date to ensure clearance, and confirm the specific hold requirement with your surgical team. Emergency surgery should proceed with the anesthesiologist informed of recent Zepbound use and the aspiration risk managed with appropriate precautions.
Does Zepbound stay in your system longer at higher doses?
The half-life, approximately 5 days, does not change with dose. What changes is the absolute amount of drug in your system at the time you stop. A patient stopping from 15 mg starts from a higher plasma plateau than a patient stopping from 5 mg. The percentage cleared per 5-day interval is identical (50%), but the absolute amount remaining at Day 10 or Day 15 is proportionally higher for the higher-dose patient. In practical terms, a patient on 15 mg may experience more residual appetite suppression at Day 10 than a patient on 5 mg, not because the drug lingers longer, but because more was present to begin with. The pharmacological clearance is effectively complete for all patients by Day 25–30, regardless of dose, consistent with the Zepbound USPI’s documentation of dose-proportional linear pharmacokinetics.
What happens to weight loss when Zepbound clears?
The SURMOUNT-4 trial published in JAMA (December 2023) is the definitive answer: patients who stopped tirzepatide after achieving a mean 20.9% weight loss regained an average of +14.0% body weight over the subsequent 52 weeks, compared to an additional −5.5% for patients who continued. Only 16.6% of patients who stopped maintained ≥80% of their lead-in weight loss at 52 weeks, versus 89.5% of continuers, per the PubMed abstract. This weight regain begins as tirzepatide clears and appetite returns, typically within the first two weeks post-last-dose. Obesity is a chronic condition that tirzepatide manages but does not cure. The clinical implication: stopping Zepbound requires a transition plan, whether that is continued behavioral intervention, dietary adjustment, or a provider-supervised dosing strategy.