

Foods to Skip vs. Foods to Emphasize on Zepbound
Tirzepatide slows gastric emptying, the wrong foods stay in your stomach longer, amplifying every GI side effect and blunting your results. Focus on lean protein, moderate fiber (after the first 4–8 weeks), low-fat foods, and non-carbonated fluids. Avoid fried foods, alcohol, refined carbs, sugary drinks, carbonated beverages, and overly large meals. The changes matter most on injection day and through the first week at each new dose level.
Why What You Eat Matters More on Zepbound Than on Most Medications
Most medications don’t change how quickly food moves through your stomach. Zepbound does, dramatically. That makes your food choices directly relevant to how you feel and how well the medication works.
How Tirzepatide Changes Your Digestion
Tirzepatide, the active ingredient in Zepbound, is a dual agonist of the GIP receptor (GIPR) and the GLP-1 receptor (GLP-1R), the first FDA-approved medication to activate both incretin pathways simultaneously. This dual mechanism is what gives tirzepatide its potency, but it also produces a GI profile that differs from single-pathway drugs.
Both the GIP and GLP-1 receptors are involved in slowing gastric emptying, the rate at which food moves from your stomach into the small intestine. When tirzepatide activates both receptors concurrently, the gastric-emptying slowdown is more pronounced than with GLP-1-only agents like semaglutide. According to the Zepbound prescribing information, tirzepatide suppresses glucagon, stimulates glucose-dependent insulin secretion, and slows gastric emptying — mechanisms that collectively reduce caloric intake and promote weight loss.
The clinical result: food you eat stays in your stomach significantly longer than it did before you started Zepbound. That sustained gastric fullness is part of how the medication suppresses appetite. It is also why the wrong meal choices produce outsized nausea, bloating, belching, and vomiting compared to a person not on tirzepatide.
Tirzepatide reaches peak plasma concentration (Tmax) between 8 and 72 hours after each subcutaneous injection, per Zepbound prescribing information. This window, when gastric slowing is at its most pronounced, is when dietary choices carry the greatest consequence.
Why Dietary Choices Amplify or Reduce Side Effects
The Zepbound FDA prescribing information adverse events table reports the following GI adverse reaction rates in the pooled SURMOUNT-1 and SURMOUNT-2 studies (placebo-controlled, Studies 1 and 2 combined):
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation | 5% | 17% | 14% | 11% |
These rates are not fixed — they represent what patients on average experience. Dietary behavior can push individual risk higher or lower within this distribution. Specifically:
- High-fat meals further slow the gastric emptying that tirzepatide has already slowed, extending the duration of nausea and increasing the likelihood of vomiting.
- Excess insoluble fiber in the early weeks — when gut motility is adjusting — increases diarrhea risk by adding bulk to a GI tract whose transit patterns have already been disrupted.
- Refined carbohydrates and sugary foods drive blood glucose spikes that partially counteract tirzepatide’s glucose-dependent insulin secretion mechanism — undermining a core pharmacological benefit.
- Large meal volume causes prolonged gastric distension when the stomach is already emptying slowly, producing the uncomfortable “too full for too long” sensation that many patients describe.
- Carbonated beverages increase gastric volume acutely, worsening bloating and abdominal discomfort.
Understanding the mechanism means understanding why these are real clinical recommendations, not generic “eat healthy” advice. The FDA approval for Zepbound on November 8, 2023 specified its use as an adjunct to a reduced-calorie diet — dietary modification is not optional, it is part of the approved treatment framework.
Foods to Avoid on Zepbound
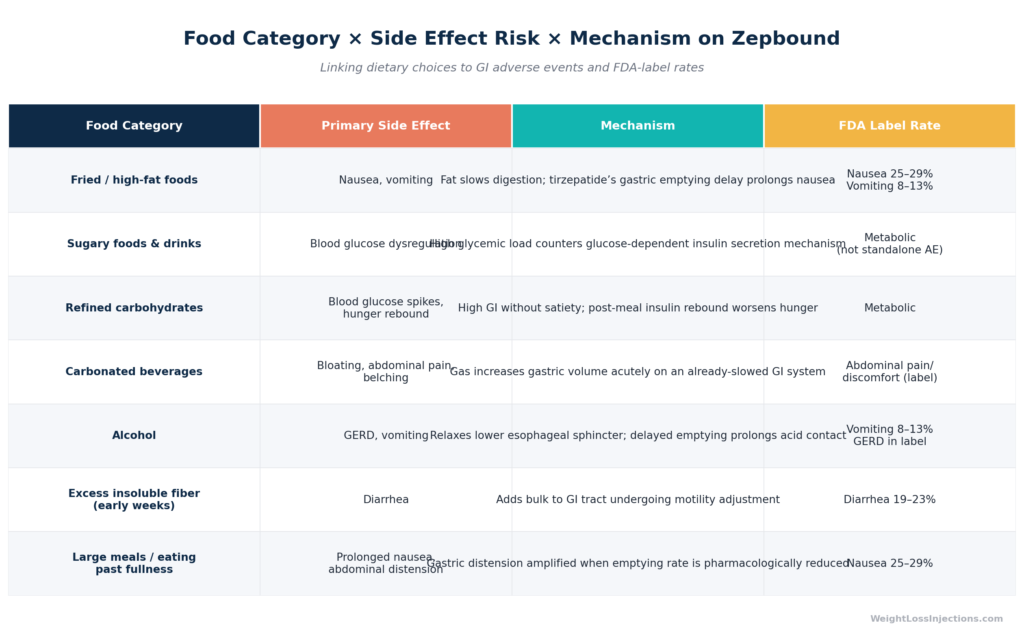
Food Category × Side Effect Risk × Mechanism on Zepbound
1. Fried and High-Fat Foods
Fat is the slowest macronutrient to digest under normal circumstances, a high-fat meal can take 4–5 hours to clear the stomach. When tirzepatide is further slowing that process, a greasy meal can sit in your stomach for an uncomfortable and nausea-inducing stretch of time.
Eli Lilly’s guidance in the Zepbound prescribing information specifically recommends avoiding fatty, greasy foods as one of the primary strategies for managing nausea. This is one of the most concrete dietary recommendations directly in the FDA label, not inferred advice.
Foods to avoid in this category:
- French fries, onion rings, fried chicken
- Bacon, processed sausage, heavily marbled red meat
- Butter-heavy sauces, cream-based pasta dishes, hollandaise
- Full-fat cheese in large amounts, heavy cream
- Fast food meals combining multiple high-fat elements
This does not mean eliminating all fat. Healthy fats in small portions, half an avocado, a small handful of almonds, a teaspoon or two of olive oil, are appropriate and nutritionally valuable. The concern is with large-fat-load meals that overwhelm a stomach that is emptying at a fraction of its pre-medication rate.
2. Sugary Foods and Drinks
Tirzepatide’s dual mechanism includes glucose-dependent insulin secretion, meaning the medication amplifies insulin release in response to blood glucose elevation. When you consume high-glycemic foods, you produce sharp glucose spikes that partially defeat one of the medication’s intended metabolic functions.
For patients with type 2 diabetes as a comorbidity, this matters more acutely. SURMOUNT-2, published in the Lancet in 2023, demonstrated that tirzepatide at 15 mg reduced HbA1c by 2.08 percentage points in T2D patients — a benefit that dietary sugar undermines by continuously loading the glycemic system the medication is working to regulate.
Foods to minimize or avoid:
- Regular soda, fruit juice, energy drinks, sweetened iced tea
- Candy, cookies, cakes, pastries, donuts
- Ice cream, sweetened yogurt, flavored granola
- Sweetened cereals, instant oatmeal with added sugar
- Syrups, honey, agave in large amounts
Diet sodas avoid the sugar, but are carbonated (see section 4 below) and should still be limited.
3. Refined Carbohydrates
Refined carbohydrates, stripped of their fiber content during processing, behave metabolically like sugar: rapid digestion, blood glucose spikes, and a quick return of hunger without the satiety that complex carbohydrates provide. On Zepbound, this is doubly counterproductive: you are taking a medication designed to suppress appetite, and refined carbs undermine that mechanism by triggering hunger rebound faster than whole-food alternatives.
Foods to reduce:
- White bread, white rice, white pasta
- Bagels, crackers without significant fiber content
- Instant mashed potatoes, most commercial breakfast cereals
- Pizza dough (standard), flour tortillas
Swap to whole-grain equivalents: brown rice, quinoa, oatmeal, whole-grain bread, lentil pasta. The transition also improves satiety, which complements tirzepatide’s appetite-suppression effect.
4. Carbonated Beverages
Carbonation introduces CO₂ gas into the GI tract. Under normal gastric function, this produces temporary bloating. On tirzepatide, with gastric emptying already slowed, that gas has nowhere to go quickly, resulting in prolonged distension, belching, and abdominal discomfort.
Notably, this applies to unsweetened sparkling water, not just soda. Some patients tolerate moderate carbonated water, but many find that any carbonation worsens their bloating, particularly in the first days after each injection. Plain still water and herbal teas are the safest substitutes.
Beverages to avoid:
- Regular soda (adds sugar issue on top of carbonation)
- Diet soda (carbonation + potential appetite-stimulating effect from artificial sweeteners)
- Sparkling water (La Croix, Perrier, club soda)
- Beer (carbonated + alcohol; the worst combination for GI comfort on Zepbound)
5. Alcohol
Alcohol warrants its own category because it introduces multiple simultaneous problems:
GERD and esophageal risk. Tirzepatide slows gastric emptying, which already creates upward pressure on stomach contents. Alcohol relaxes the lower esophageal sphincter, the valve that keeps stomach acid from entering the esophagus. The Zepbound prescribing information lists GERD as a recognized adverse event. Adding alcohol to an already-slowed stomach compounds acid reflux risk significantly.
Caloric interference. Alcohol delivers approximately 7 calories per gram, more than carbohydrates or protein, with no satiety effect and no nutritional value. For patients using tirzepatide to achieve a caloric deficit, alcohol is among the least efficient ways to spend caloric budget.
Hypoglycemia risk for T2D patients. If you have type 2 diabetes and are using insulin or a sulfonylurea alongside tirzepatide, alcohol can precipitate hypoglycemia by blunting hepatic glucose production. The Zepbound prescribing information highlights hypoglycemia risk when tirzepatide is combined with insulin or sulfonylurea agents, alcohol amplifies this risk.
For the full clinical picture on alcohol and Zepbound, see the dedicated guide at WeightLossInjections.com (alcohol-and-zepbound).
6. High-Fiber Foods — In Early Weeks Only
This recommendation is time-limited and important to understand correctly: dietary fiber is beneficial long-term and should be part of a Zepbound-compatible eating pattern. The concern applies specifically to large amounts of insoluble fiber during the first 4–8 weeks on the medication.
Tirzepatide alters gut motility. As the GI tract adjusts, insoluble fiber — which adds bulk and affects transit time — can contribute to the diarrhea that affects 19–23% of patients, per the Zepbound prescribing information adverse events table.
Foods to moderate temporarily (first 4–8 weeks):
- Raw cruciferous vegetables in large amounts (broccoli, cauliflower, Brussels sprouts, cabbage)
- Bran cereals, high-fiber granola
- Large servings of beans and lentils
- Apple skins, raw pear, other high-skin-fiber fruits
After the initial adjustment period, reintroduce these foods gradually. Long-term fiber intake supports bowel regularity, cardiovascular health, and the satiety that complements Zepbound’s weight management mechanism.
7. Large Meals and Eating Past Fullness
This is not about a specific food category but a behavioral pattern that tirzepatide makes genuinely hazardous to comfort. When gastric emptying is pharmacologically slowed, overeating means prolonged gastric distension, a full-stomach sensation that can last hours rather than the 30–60 minutes it might take to resolve under normal digestion.
Tirzepatide also acts on hypothalamic satiety pathways, enhancing the “I’m full” signal. Patients who override this signal — eating past comfort because the food tastes good or because the portion looks normal, are working against the medication’s mechanism and typically pay for it with hours of nausea.
Practical behavioral guidance:
- Stop eating at 70–80% of your previous “full” threshold
- Take 20 minutes or longer per meal — gastric stretch receptors take time to signal the brain
- Use smaller plates and pre-portion meals rather than eating from serving containers
- Wait at least 15 minutes before deciding to have seconds
What to Eat on Zepbound: The Recommended Plate
Knowing what to avoid is only half the picture. SURMOUNT-1, published in the New England Journal of Medicine in 2022 by Jastreboff et al., enrolled participants on a reduced-calorie diet alongside tirzepatide, the trial that produced the pivotal 15–21% weight loss results was not medication-only. The dietary component matters.
Lean Proteins: Prioritize at Every Meal
Tirzepatide drives caloric restriction, and caloric restriction without adequate protein preferentially degrades lean muscle mass. Preserving muscle is critical: it supports metabolic rate, functional strength, and body composition outcomes that the scale does not capture.
Target 25–30 grams of protein per meal. Good sources that are also low-fat and GI-friendly:
- Chicken breast and turkey breast (baked, grilled, or poached — not fried)
- White fish (cod, tilapia, halibut) and salmon (higher fat but nutrient-dense in small amounts)
- Eggs and egg whites
- Greek yogurt (plain, low-fat) and cottage cheese
- Legumes (moderate amounts after adjustment period) — black beans, edamame, lentils
Non-Starchy Vegetables
Non-starchy vegetables provide micronutrients, moderate fiber, and volume with minimal caloric density. In the early weeks, cooked vegetables are easier on the GI tract than raw, steamed spinach, sautéed zucchini, roasted green beans, and cooked tomatoes are all appropriate.
As tolerance improves (typically after weeks 4–8), reintroduce raw vegetables gradually. Leafy salad greens (lettuce, arugula, cucumber) are generally well-tolerated even early on because they are low in insoluble fiber.
Whole Grains and Complex Carbohydrates
Choose carbohydrate sources that provide fiber, slow glucose absorption, and maintain satiety longer than their refined counterparts:
- Oatmeal (steel-cut or rolled — not instant with added sugar)
- Quinoa
- Brown rice (moderate portions — a half cup cooked is appropriate)
- Sweet potato in moderate amounts
- Whole-grain bread (look for ≥2 g fiber per slice, whole grain as first ingredient)
Healthy Fats — Small Amounts
Fat is not eliminated on Zepbound — it is moderated. Small amounts of unsaturated fats provide satiety, support fat-soluble vitamin absorption, and contribute to overall dietary quality:
- Half an avocado per serving (not a full one)
- Olive oil for cooking: 1–2 teaspoons
- Nuts: a small closed handful, not a bowl
- Natural nut butters: 1–2 tablespoons
Avoid combining multiple fat sources at the same meal — even healthy fats in large cumulative amounts slow gastric emptying.
Hydration Strategy
GI adverse effects — diarrhea and vomiting in particular — create real fluid loss risk. The Zepbound prescribing information identifies dehydration leading to acute kidney injury as a precaution requiring adequate hydration. Aim for 8–10 glasses of still water daily.
Critical hydration protocol:
- Drink fluids between meals rather than with large amounts of food — drinking heavily with a meal compounds gastric fullness on an already-slowed system
- Herbal teas (ginger, peppermint) are well-tolerated and may actively reduce nausea
- Low-sugar electrolyte drinks (LMNT, Liquid IV diluted, coconut water in small amounts) can help replenish electrolytes lost to diarrhea or vomiting
- Broth-based soups count toward fluid intake and provide sodium, which matters during acute GI fluid losses
- Avoid sugary sports drinks — the glucose load works against tirzepatide’s glycemic mechanism
Injection Day Diet Strategy
Day of Injection
The 8–72 hour Tmax window for tirzepatide — per Zepbound prescribing information — means the period immediately surrounding your injection is when gastric slowing is ramping up most sharply. This is the highest-risk window for dietary-induced nausea.
On injection day:
- Eat a light, low-fat meal 1–2 hours before or after your injection
- Preferred foods: plain oatmeal, scrambled eggs, toast with a thin spread, broth-based soup, plain rice with steamed vegetables
- Keep portion sizes smaller than usual — 50–70% of a normal meal
- Avoid the foods on the “skip” list above — particularly fatty, fried, or carbonated items
- Stay well-hydrated with still water or herbal tea
Zepbound can be taken at any time of day with or without food per Zepbound dosing guidance from Eli Lilly. That flexibility is useful — some patients inject in the morning when their stomach is already light from overnight fasting, reducing the chance that food choices immediately worsen nausea.
Days 2–5 Post-Injection: The Peak GI Effect Window
Nausea and GI side effects typically peak in the first 2–5 days after each injection, particularly at the start of treatment or after each dose escalation. During this window:
- Eat 4–5 smaller meals rather than 2–3 larger ones
- Maintain the low-fat, low-fiber, high-protein approach from injection day
- Keep carbonated beverages and alcohol strictly off the table
- If nausea is present, focus on bland foods: plain crackers, toast, plain rice, banana, broth
- Resume more variety from day 6 onward, while maintaining the long-term Zepbound-compatible eating pattern
Zepbound Diet at Each Dosing Stage
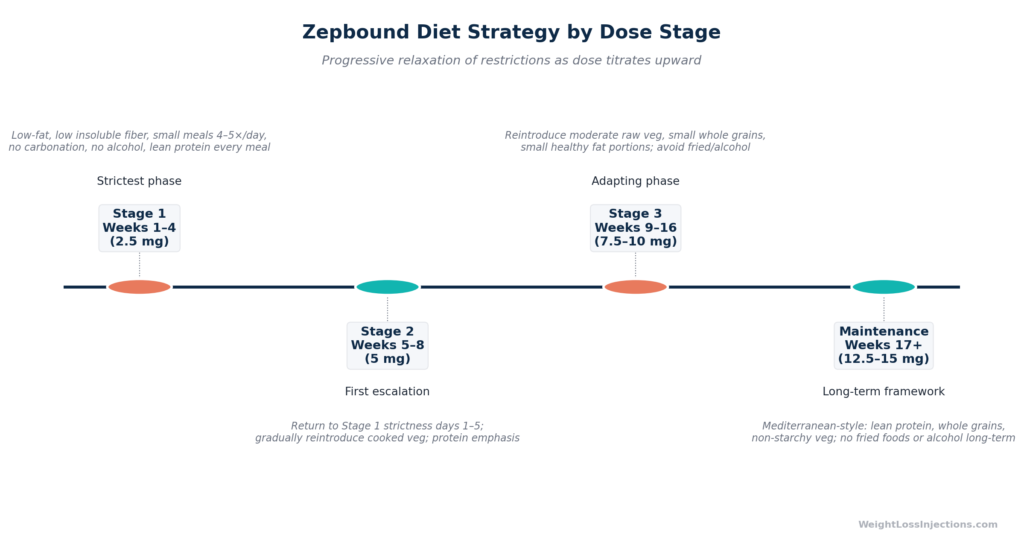
Zepbound Diet Strategy by Dose Stage
The standard Zepbound titration begins at 2.5 mg once weekly for 4 weeks, then increases by 2.5 mg every ≥4 weeks through the sequence: 2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg, per Zepbound prescribing information. Each dose escalation partially resets the GI adjustment clock — the first several days at a new dose level often bring back nausea and GI sensitivity similar to the first weeks.
Weeks 1–4 (2.5 mg — initiation): Apply the strictest dietary approach. The GI tract is adjusting from baseline. Small meals, low fat, low insoluble fiber, no carbonation, no alcohol. Lean protein at every meal. This is temporary, not permanent.
Weeks 5–8 (5 mg — first escalation): The GI symptoms that may have settled at 2.5 mg can return for days 1–7 after the dose increase. Treat days 1–7 of the 5 mg phase like the strictest weeks of initiation, then gradually liberalize as tolerance builds.
Weeks 9–16 (7.5–10 mg): Most patients see meaningful GI adaptation by this point. You can reintroduce moderate amounts of raw vegetables, a wider variety of whole-grain foods, and a broader range of textures. Continue to avoid fried food, alcohol, and refined carbs — not because they are still causing acute GI symptoms for everyone, but because they actively undermine the weight management goal.
Maintenance (12.5–15 mg): A Mediterranean-style dietary pattern aligns well with tirzepatide’s metabolic profile — it naturally emphasizes lean proteins, vegetables, olive oil in moderate amounts, whole grains, and legumes. The long-term avoidances remain fried food and alcohol, which offer no benefit and carry continued GI and metabolic risk.
Our take at WeightLossInjections.com: Most patients who struggle with Zepbound nausea in the first 4–8 weeks are inadvertently making it worse through diet — not because they are ignoring instructions, but because the connection between a specific meal and several hours of subsequent nausea is not always obvious until someone explains the mechanism. Tirzepatide’s dual GIP/GLP-1 action creates a gastric-emptying slowdown that is more pronounced than many patients expect. The payoff for eating carefully is real: fewer side effects, better medication adherence, and a diet that works with tirzepatide’s appetite-suppression mechanism rather than against it. If you want personalized dietary guidance alongside your prescription, WeightLossInjections.com offers a bundled telehealth program at [$X/month] that includes [service detail] — a licensed provider who can adapt your dietary recommendations as you move through the titration schedule.
Frequently Asked Questions
What foods should I avoid on injection day for Zepbound?
On injection day, avoid fatty foods (fried items, heavy sauces, bacon, cream-based dishes), carbonated beverages, alcohol, and large portions of any food. Tirzepatide reaches peak plasma concentration 8–72 hours after injection, per the Zepbound prescribing information, meaning the gastric-emptying slowdown intensifies in the hours and days immediately following your dose. Light, low-fat, easily digestible foods, plain oatmeal, scrambled eggs, toast, broth — minimize GI distress during this peak window.
Can I eat fatty foods on Zepbound?
Large, high-fat meals should be avoided throughout tirzepatide treatment, but especially in the first weeks and around each injection. Fat is the slowest macronutrient to digest, and tirzepatide further slows gastric emptying — the combination keeps food in your stomach much longer than normal, prolonging nausea and increasing vomiting risk. Small amounts of healthy unsaturated fats (half an avocado, a tablespoon of olive oil, a small handful of nuts) are appropriate and part of a balanced Zepbound-compatible diet. Fried foods, butter-heavy dishes, and high-fat processed meats should be minimized long-term, as explicitly recommended in the Zepbound prescribing information.
Is alcohol safe to drink while taking Zepbound?
Alcohol is not prohibited outright in the Zepbound label, but it is inadvisable for several reasons. Tirzepatide already increases the risk of GERD — listed as an adverse event in the Zepbound prescribing information — and alcohol relaxes the lower esophageal sphincter, compounding acid reflux risk when the stomach is already emptying slowly. Alcohol also contributes empty calories that directly undermine the caloric deficit Zepbound is designed to create. For patients with T2D using insulin or a sulfonylurea alongside tirzepatide, alcohol adds hypoglycemia risk. For a full discussion, see the alcohol-and-zepbound guide at WeightLossInjections.com.
Why does eating high-fiber food cause diarrhea on Zepbound?
Insoluble fiber adds bulk to stool and affects intestinal transit time. When tirzepatide alters gut motility during the adjustment period, particularly in the first 4–8 weeks, adding large amounts of insoluble fiber can disrupt transit patterns unpredictably, contributing to the diarrhea that affects 19–23% of Zepbound patients across the dose range, per the Zepbound prescribing information adverse events table. This is a temporary consideration: after the GI tract adjusts, reintroducing fiber gradually is recommended, as long-term dietary fiber supports bowel regularity, cardiovascular health, and sustained satiety.
What should I eat if I feel nauseous after my Zepbound injection?
Nausea after a Zepbound injection responds well to the BRAT-adjacent approach: bland, low-fat, low-fiber foods in small portions. Plain crackers, toast, plain white rice, banana, broth, and plain oatmeal are consistently well-tolerated. Cold or room-temperature foods tend to be easier than hot meals, which have stronger aromas. Ginger tea (unsweetened) has evidence for mild nausea relief and is safe alongside tirzepatide. Eating every 3–4 hours in small amounts rather than waiting until very hungry prevents the empty-stomach nausea that can compound drug-related symptoms. For persistent vomiting that prevents adequate hydration, contact your prescribing provider, the Zepbound prescribing information notes that fluid losses from GI adverse events can lead to acute kidney injury if hydration is not maintained.
Do I need to follow a specific diet for Zepbound to work?
The FDA indication for Zepbound specifies it as an adjunct to a reduced-calorie diet and increased physical activity — meaning diet and exercise are part of the approved treatment, not optional add-ons. The SURMOUNT-1 trial that supported approval enrolled participants on a reduced-calorie diet alongside tirzepatide. No specific diet is mandated, but the dietary principles in this article — high lean protein, low fat, moderate fiber after adjustment, no alcohol, no refined carbs, non-carbonated fluids — reduce side effects and optimize the metabolic environment tirzepatide is working within. Patients who make these changes typically experience fewer GI symptoms and better adherence, which translates to better long-term outcomes.
This article is for educational purposes only and does not constitute medical advice. Zepbound is FDA-approved as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management. Dietary recommendations are general guidance; consult a licensed provider for individualized advice. WeightLossInjections.com’s editorial team reviews all content quarterly; last medical review: April 2026. Weight loss results vary by individual; trial averages represent population means, not guaranteed outcomes for any individual patient.