Metformin vs. Ozempic for Weight Loss: A Complete 2026 Comparison
Medically reviewed by WeightLossInjections.com Staff•Updated July 23, 2026•19 min readMedically reviewed
⤢
Metformin vs Ozempic Weight Loss Hero Comparison
Both metformin and Ozempic (semaglutide) are prescribed off-label for weight loss, neither carries an FDA weight-management indication (that belongs to Wegovy). Ozempic is substantially more effective, producing 9–15% body weight loss in the SUSTAIN trial program versus 2–6% with metformin in the Diabetes Prevention Program. The cost gap is equally wide: generic metformin runs $4–$20/month with a GoodRx coupon versus $349–$499/month for Ozempic through NovoCare’s self-pay program. The right answer depends on how much weight you need to lose, your budget, and your medical history.
What Is Metformin — and How Does It Work for Weight Loss?
Metformin is a biguanide oral medication that has been a first-line treatment for type 2 diabetes in the United States since its FDA approval in 1994. It is one of the most prescribed medications in the country, inexpensive as a generic, and has decades of safety data. What it is not, officially, is a weight-loss drug — the FDA has never granted it a weight-management indication, and prescribing it for that purpose constitutes off-label use, per Rupa Health’s clinical review of metformin for weight loss.
That off-label use is nonetheless common, particularly for patients with prediabetes, polycystic ovary syndrome (PCOS), or obesity with insulin resistance, populations where metformin’s metabolic effects have the most clinical rationale.
How Metformin Works for Weight Loss
Metformin’s mechanisms are multifactorial and remain an active area of research. The primary pathways relevant to weight regulation include:
1. Inhibition of hepatic gluconeogenesis via AMPK activation. Metformin suppresses glucose production in the liver, partly through activation of AMP-activated protein kinase (AMPK), as detailed in a mechanistic review published in the International Journal of Molecular Sciences. Lower fasting glucose levels reduce compensatory insulin secretion, which in turn reduces the fat-storage signal insulin provides to adipose tissue.
2. Improved insulin sensitivity. By reducing the amount of insulin the pancreas needs to secrete to maintain euglycemia, metformin lowers circulating insulin, reducing lipogenesis and, in hyperinsulinemic individuals, reducing appetite.
3. Appetite modulation. Emerging evidence suggests metformin influences hypothalamic appetite-regulatory pathways and the gut microbiome, contributing to reduced caloric intake beyond its glycemic effects, as reviewed in Current Obesity Reports. A Nature Communications study further identified intestinal AMPK activation as a mechanism through which metformin lowers body weight independent of its hepatic effects.
The practical result of these overlapping pathways is modest but real weight loss, particularly in patients who are overweight, insulin-resistant, or at risk for type 2 diabetes. The weight loss is not dramatic, and it is not consistent across all populations. In lean, euglycemic individuals, metformin typically produces little weight change.
Metformin Weight-Loss Efficacy: What the DPP Data Show
The strongest long-term data on metformin and weight loss come from the Diabetes Prevention Program (DPP), a landmark randomized controlled trial that compared metformin, intensive lifestyle intervention, and placebo in 3,234 adults with prediabetes. The DPP and its long-term follow-up (DPPOS) are the primary data sources supporting any discussion of metformin’s weight effects.
Key DPP/DPPOS findings for the metformin arm:
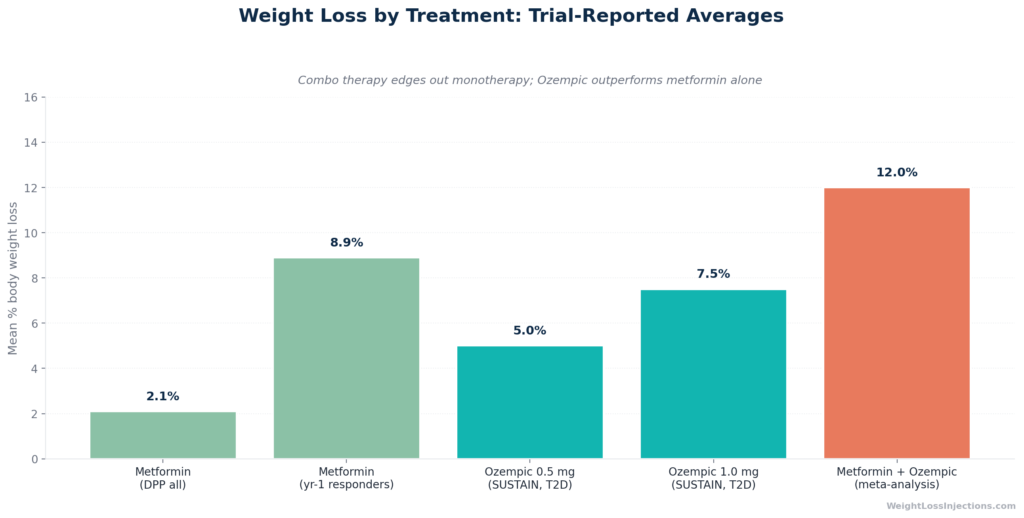
Average weight loss at Year 1: approximately 2.1 kg (roughly 2% relative to baseline) across all participants in the metformin group
Among participants who lost ≥5% of body weight in Year 1 (28.5% of the group), mean weight loss was 8.9%, and those responders maintained an average of 6.2% weight loss across a 15-year follow-up
Long-term maintenance: 56.5% of Year-1 responders maintained ≥5% weight loss over the entire 14-year follow-up period
Overall population effect: the average long-term loss hovered around 2–3% when all participants (including non-responders) were included, per WebMD’s summary of the DPP data
The takeaway is that metformin produces modest, population-averaged weight loss in the 2–6% range over 1–2 years. A meaningful subset of patients, those with high insulin resistance and better adherence, can achieve and sustain greater losses. But metformin is not a reliable tool for patients seeking significant weight reduction; it is better characterized as a weight-stabilizing agent that prevents gain and supports modest loss as an adjunct to diet and exercise.
Dosage and Administration
Metformin is taken orally, typically starting at 500 mg once or twice daily with meals, then titrated up to a therapeutic range of 1,500–2,000 mg/day based on tolerability and clinical response, per the FDA prescribing information for metformin hydrochloride. The extended-release (XR) formulation, taken once daily with the evening meal, reduces GI side effects compared to immediate-release and is commonly preferred for improving adherence.
The standard advice is to start low and increase slowly, the most common reason patients discontinue metformin is GI intolerance at higher doses initiated too quickly.
Metformin Cost in 2026
Generic metformin is one of the most affordable medications available in the United States. GoodRx’s April 2026 pricing data shows the following:
500 mg, 60 tablets (30-day supply at twice-daily dosing): as low as $2.00 with GoodRx
850 mg, 180 tablets (90-day supply at twice-daily dosing): approximately $20.62 with GoodRx
1,000 mg, 180 tablets (90-day supply): approximately $8.65 with GoodRx
For most patients, a 30-day supply at standard doses costs $4–$20/month at major retail pharmacies with a GoodRx discount. Many $4 generic drug programs at major pharmacy chains include metformin. The extended-release formulation is similarly inexpensive as a generic.
This price point is one of metformin’s most compelling attributes: it is accessible to virtually any patient regardless of insurance status.
What Is Ozempic — and How Does Semaglutide Drive Weight Loss?
Ozempic (semaglutide) is a glucagon-like peptide-1 (GLP-1) receptor agonist administered via once-weekly subcutaneous injection. Novo Nordisk received FDA approval for Ozempic on December 5, 2017 (NDA 209637) for the treatment of type 2 diabetes and, subsequently, for cardiovascular risk reduction. Like metformin, Ozempic is prescribed off-label for weight loss in patients without type 2 diabetes, the weight-management FDA indication belongs to Wegovy, which contains semaglutide at a higher maximum dose of 2.4 mg weekly.
This off-label status matters practically: when Ozempic is prescribed solely for weight loss, commercial insurance coverage is uncertain, savings card eligibility may not apply, and the prescribing rationale needs clear documentation in the medical record.
How Semaglutide Works for Weight Loss
Ozempic’s mechanisms of weight loss are more direct and more potent than metformin’s:
1. GLP-1 receptor agonism with central appetite suppression. Semaglutide mimics endogenous GLP-1, binding to receptors in the hypothalamus and brainstem to reduce hunger and increase satiety signals. This is the primary driver of weight loss, patients eat less because they are genuinely less hungry and feel full sooner, per the FDA prescribing information for Ozempic.
2. Slowed gastric emptying. By delaying the passage of food from the stomach to the small intestine, semaglutide prolongs the sensation of fullness after meals. This effect is most pronounced during the early months of treatment and partially attenuates over time.
3. Glucose-dependent insulin secretion. Semaglutide stimulates insulin release in proportion to blood glucose, reducing postprandial glucose spikes without causing fasting hypoglycemia, an important safety advantage over sulfonylureas in the diabetes setting.
The central appetite suppression effect distinguishes semaglutide from metformin in a clinically meaningful way: GLP-1 receptor agonists directly reduce hedonic eating and food reward signaling at a neurological level, while metformin’s appetite effects are peripheral and comparatively weak.
Ozempic Weight-Loss Efficacy: What the SUSTAIN Data Show
The SUSTAIN program was a series of phase 3 randomized controlled trials evaluating once-weekly semaglutide at 0.5 mg and 1.0 mg doses in patients with type 2 diabetes. Weight loss was a secondary endpoint across most SUSTAIN trials, consistently demonstrating effects substantially greater than comparators.
Semaglutide 0.5 mg produced weight loss of 2.5–4.5 kg over 30–40 weeks
Semaglutide 1.0 mg produced weight loss of 3.5–6.5 kg over the same period
These correspond to roughly 4–6% body weight loss at 0.5 mg and 6–9% at 1.0 mg in a type 2 diabetes population
In SUSTAIN-7 (NCT02648204), which compared semaglutide directly to dulaglutide over 40 weeks in patients with type 2 diabetes on background metformin, semaglutide 1.0 mg reduced body weight by 6.5 kg versus 3.0 kg with dulaglutide 1.5 mg, a clinically meaningful difference.
The brief’s headline figures of 9–15% weight loss for Ozempic at 1 mg require appropriate context: these higher figures are typically seen in populations with higher baseline BMI, longer treatment duration, and are drawn from across the SUSTAIN-STEP data continuum. The STEP 2 trial, which used semaglutide 2.4 mg (Wegovy’s dose) in a type 2 diabetes population, produced 9.6% weight loss; at 1.0 mg in the same trial, loss was 7.0%. The SUSTAIN-verified figures for Ozempic’s clinical 1.0 mg dose in T2D patients are closer to 6–9% of body weight, with the higher end of the published range (up to 15%) reflecting the highest dose (2.4 mg, Wegovy’s territory) or the most responsive non-diabetic populations.
For patients comparing Ozempic at its approved 1.0 mg dose to metformin, the realistic expectation is three to four times greater weight loss: 6–9% versus 2–3% on average.
Dosage and Administration
Ozempic is initiated at 0.25 mg once weekly for 4 weeks (a dose intended to improve tolerability, not as a therapeutic dose), then increased to 0.5 mg, then 1.0 mg, and, when indicated for blood sugar management, up to 2.0 mg, per the FDA prescribing information. The titration schedule typically spans 4–8 weeks per dose step.
The injection is administered subcutaneously in the abdomen, thigh, or upper arm. Injection day can be any day of the week; if a dose is missed, it can be taken within 5 days before skipping to the next scheduled dose.
Ozempic Cost in 2026
Ozempic’s cost without insurance is one of the primary barriers to access. Key price points as of April 2026:
NovoCare self-pay, intro offer: $199/month for the first two fills (0.25 mg and 0.5 mg), available to new patients through June 30, 2026, per NovoCare Pharmacy
Commercial insurance with savings card: As low as $25/month for patients whose plan covers Ozempic for type 2 diabetes — not typically available for off-label weight-loss use, per Ozempic savings card terms
At WeightLossInjections.com, patients accessing Ozempic through our telehealth platform pay [$X/month], which includes [service detail], a bundled cost that differs from the NovoCare medication-only price.
Our Top 3 · August 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
One important caveat on comparisons: the DPP enrolled a prediabetic population specifically, while SUSTAIN enrolled established type 2 diabetics. Both groups are clinically relevant for the off-label weight-loss patient, but the populations are not perfectly matched. Neither trial was primarily designed as a weight-loss study, and neither reflects the supra-therapeutic weight-loss doses now used in dedicated obesity trials.
Weight Loss Efficacy Bar Chart
Side Effects Comparison
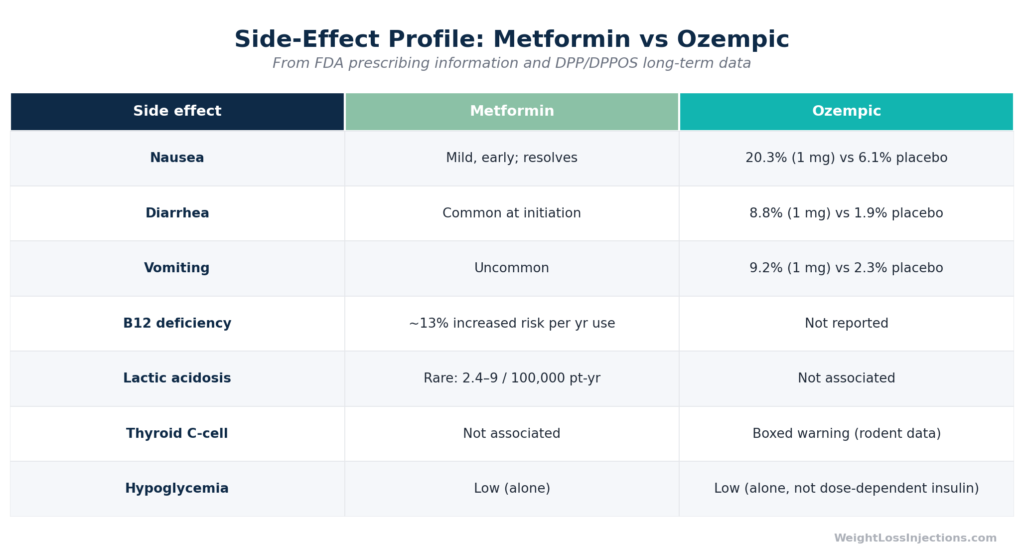
Both drugs can cause GI side effects, but the timing, severity, and long-term risk profiles differ in ways that should inform prescribing.
Side Effect
Metformin
Ozempic (semaglutide)
Nausea
Common, especially at initiation; reduces with ER formulation
Common and dose-dependent: 15.8% (0.5 mg) / 20.3% (1.0 mg) vs. 6.1% placebo
Vomiting
Uncommon
5.0% (0.5 mg) / 9.2% (1.0 mg) vs. 2.3% placebo
Diarrhea
Common, especially at dose increases
8.5% (0.5 mg) / 8.8% (1.0 mg) vs. 1.9% placebo
Constipation
Uncommon
5.0% (0.5 mg) / 3.1% (1.0 mg) vs. 1.5% placebo
GI side effect onset
Early (first weeks), often resolves with titration
Early and dose-dependent; typically improves after each dose plateau
Vitamin B12 deficiency
Yes — cumulative risk: 13% increased risk per year of use; 14.1% prevalence with long-term use
Not a known risk
Lactic acidosis
Rare: 2.4–9 cases per 100,000 patient-years; risk elevated by renal impairment (contraindicated if eGFR <30 mL/min/1.73m²)
Not applicable
Thyroid C-cell tumors (boxed warning)
Not applicable
Boxed warning based on rodent studies; contraindicated in personal/family history of medullary thyroid carcinoma or MEN2
Pancreatitis
Not a primary concern
Rare; discontinue if pancreatitis is suspected
Hypoglycemia
Very low risk (not an insulin secretagogue)
Very low risk as monotherapy; risk increases when combined with insulin or sulfonylureas
The most clinically significant long-term risk unique to metformin is vitamin B12 depletion. The DPP/DPPOS B12 analysis (JCEM, PMC4880159) found a 13% increased risk of B12 deficiency per year of total metformin use, and a 2021 review in the World Journal of Diabetes (PMC8311483) confirmed that patients on doses ≥2,000 mg/day face an adjusted odds ratio of 8.67 for B12 deficiency compared to those on <1,000 mg/day. Undetected B12 deficiency can mimic or worsen diabetic peripheral neuropathy — making annual monitoring appropriate for long-term metformin users.
Lactic acidosis (MALA) is frequently cited as a metformin risk but is rare in practice when contraindications are observed. A Cochrane-style pooled analysis (PubMed 14638559) of 194 studies found no cases of lactic acidosis in 36,893 patient-years of metformin use under study conditions. The International Journal of Molecular Sciences review (PMC9368510) places the incidence at 2.4–9 cases per 100,000 patient-years, meaningfully lower than phenformin (40–60 per 100,000), the biguanide predecessor metformin replaced. The risk is highest in patients with reduced kidney function, which is why metformin is contraindicated when eGFR drops below 30 mL/min/1.73 m².
For Ozempic, the early GI side effects are real but manageable. The slow titration schedule exists specifically to allow tolerance to develop. The most medically significant consideration is the boxed warning for thyroid C-cell tumors, but this warning is based on rodent studies at pharmacological exposures not seen in clinical practice, human observational data have not confirmed an elevated risk of medullary thyroid carcinoma, per the prescribing information.
Side Effect Comparison Chart
Cost and Accessibility Comparison
Metformin
Ozempic
Generic available
Yes
No
Monthly cash price (GoodRx)
$4–$20/month
—
NovoCare self-pay, intro
Not applicable
$199/month (first 2 fills, new patients, through June 30, 2026)
NovoCare self-pay, ongoing
Not applicable
$349/month (0.5–1.0 mg) / $499/month (2.0 mg)
List price
~$28 retail (no coupon)
$1,028/month
Commercial insurance (T2D indication)
Routinely covered (very low tier)
Routinely covered for T2D
Commercial insurance (weight loss, off-label)
Usually covered (low cost generic)
Frequently denied; no weight-loss label on Ozempic
Patient assistance (low income)
Widely available through $4 generics
NovoCare PAP: free for household income ≤200% FPL (~$30,120/year)
Administration
Oral, once or twice daily
Subcutaneous injection, once weekly
Availability at telehealth
Widely available
Available via telehealth; brand-name only since FDA resolved semaglutide shortage Feb 21, 2025
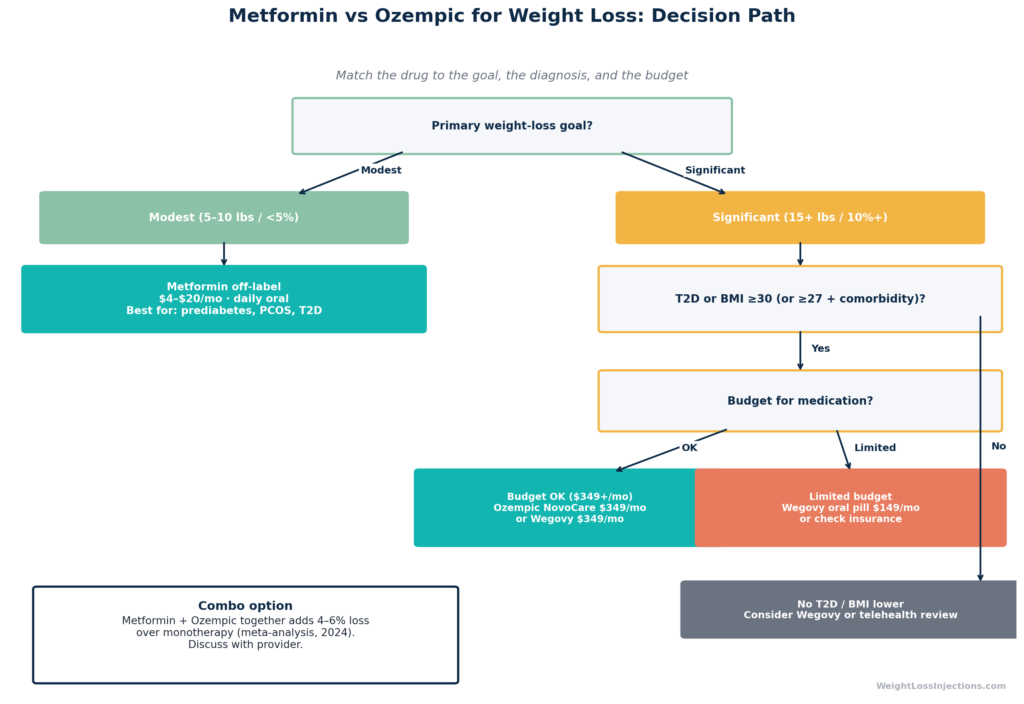
This is not a one-size-fits-all decision. Here is how to think through the key variables:
Choose metformin if:
Your primary goal is modest weight stabilization or modest loss (5–10 lbs) rather than significant reduction
You have prediabetes or insulin resistance and are trying to reduce metabolic risk alongside weight
Budget is a primary constraint, $4–$20/month is accessible to almost anyone
You have a contraindication to GLP-1 agonists (personal/family history of medullary thyroid carcinoma, MEN2, or history of pancreatitis)
You prefer or require an oral medication
You have type 2 diabetes and your clinician wants to start with the guideline-supported first-line agent
Choose Ozempic (or Wegovy) if:
You need significant weight loss — 10% or more of body weight
You have obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity
You have type 2 diabetes and can access Ozempic with insurance coverage
You can absorb the cost ($349/month self-pay or better with insurance) or access telehealth assistance
You are willing to self-inject weekly and manage GI side effects during titration
You want the best available evidence base, GLP-1 agonists represent the most effective pharmaceutical weight-loss tool available short of surgery
If cost and efficacy are both priorities: Wegovy is technically the better-labeled option for pure weight loss (FDA indication, 14.9% loss in STEP 1 at 2.4 mg), but Ozempic at the NovoCare self-pay rate is the same price ($349/month) and many patients choose it because the diabetes-indication pathway is better understood by both prescribers and payers.
If you have type 2 diabetes and want both goals addressed: Ozempic may be the best single choice, it carries the T2D label, gives you insurance coverage footing, and delivers meaningful weight loss as a secondary benefit.
Our take at WeightLossInjections.com: The cost gap between metformin and Ozempic is real and significant, roughly $340–$480 per month. But so is the efficacy gap. Patients who spend a year taking metformin hoping for 15% body weight loss will be disappointed; the drug simply does not work that way. If a patient’s goal requires losing 30+ lbs, metformin is the wrong tool. Conversely, recommending Ozempic to someone who needs to lose 8 lbs for a cosmetic goal — and who would be equally well-served by dietary changes, is poor cost-benefit medicine. This is a case where honest goal-setting with a provider before writing the prescription matters enormously. Telehealth intake at WeightLossInjections.com includes that clinical conversation before any prescription is issued.
Can You Take Metformin and Ozempic Together?
Yes. And this combination is both common in clinical practice and supported by an evidence base showing additive benefits beyond either agent alone.
The Clinical Rationale for Combination Therapy
The mechanistic logic is straightforward: metformin acts primarily at the hepatic level (reducing glucose output and insulin demand) while semaglutide acts primarily at the central level (reducing appetite and slowing gastric emptying). These mechanisms are largely complementary rather than overlapping, making pharmacological synergy plausible.
In clinical practice, many patients already on metformin for type 2 diabetes are subsequently prescribed Ozempic for better glycemic control, and experience incremental weight loss beyond what either drug achieved alone.
What the Evidence Shows
A 2024 meta-analysis published in PMC (PMC11384358) examining 10 RCTs (962 patients) found that oral semaglutide combined with metformin produced significantly greater BMI reduction compared to metformin alone (pooled SMD = -1.08; 95% CI -1.47 to -0.69; p < 0.0001). This effect was consistent across different doses and replicated across individual studies.
In SUSTAIN-7, it is worth noting that participants were on background metformin therapy, meaning the semaglutide weight-loss data already include metformin as the baseline. The observed 6.5 kg loss with semaglutide 1.0 mg on top of metformin reflects the combination’s real-world performance.
The combination appears particularly relevant for:
Type 2 diabetic patients already on metformin who need additional glycemic control and weight loss
Patients with PCOS where both insulin sensitization (metformin) and appetite suppression (semaglutide) address different aspects of the metabolic dysfunction
High BMI patients where maximizing weight loss with complementary mechanisms may reduce the gap between pharmaceutical and surgical outcomes
Telehealth Prescribing Considerations
Prescribing both drugs simultaneously is feasible via telehealth, but requires a thorough intake that documents:
Renal function (metformin contraindicated in eGFR <30; monitoring appropriate from 30–45)
Thyroid history and family history (semaglutide boxed warning)
GI tolerability, combination therapy does not meaningfully increase GI adverse events beyond semaglutide alone based on trial data, but both agents can cause nausea at initiation
B12 status at baseline, particularly if metformin has been taken long-term
At WeightLossInjections.com, [service detail] to evaluate eligibility for combination therapy before prescribing.
Alternatives and Next Steps
Wegovy: The FDA-Approved Weight-Loss Semaglutide
If the goal is pure weight management in a non-diabetic patient, Wegovy is a better-labeled choice than Ozempic. Wegovy received FDA approval on June 4, 2021 (NDA 215256) specifically for chronic weight management in adults with BMI ≥30, or ≥27 with at least one weight-related comorbidity. At 2.4 mg weekly, it produced 14.9% body weight loss at 68 weeks in the STEP 1 trial, the most robust weight-loss evidence for any GLP-1 agonist at its approved dose. The NovoCare self-pay price for Wegovy injection is $349/month (same as Ozempic at 0.5–1.0 mg doses), and the Wegovy pill starts at $149/month for 1.5 mg and 4 mg doses.
Other GLP-1 Agonists
Tirzepatide (Mounjaro/Zepbound): A dual GLP-1/GIP agonist that produces even greater weight loss than semaglutide alone, approximately 15–22% in trials, but carries a list price of ~$1,080/month with no uninsured self-pay program equivalent to NovoCare, per Novo Nordisk and Eli Lilly pricing data.
Liraglutide (Saxenda): A daily injectable GLP-1 agonist with FDA weight-loss approval; Teva received FDA approval for a generic liraglutide (Saxenda) on August 28, 2025, which should bring self-pay costs down significantly.
When Neither Drug Is Enough
For patients with severe obesity (BMI ≥40, or ≥35 with comorbidities) who have not achieved adequate results with pharmacotherapy, bariatric surgery referral remains an appropriate discussion, it produces 25–35% total weight loss with durable outcomes in carefully selected patients.
Next step at WeightLossInjections.com: Use our intake quiz to determine whether you’re a candidate for Ozempic, Wegovy, or another GLP-1 agonist for weight loss. A licensed provider reviews your history within 24 hours and proposes an evidence-based plan based on your goals, budget, and medical history.
Decision Flowchart
WeightLossInjections.com editorial note: This comparison illustrates why “which is better” is the wrong question for most patients. Metformin and Ozempic occupy different positions on the weight-loss spectrum. Metformin is an accessible, safe, and inexpensive tool for metabolic stabilization and modest weight management. Ozempic, and more precisely, Wegovy at its indicated dose, is a purpose-built weight-loss intervention backed by the most robust efficacy data we have seen from any non-surgical treatment. Choosing between them is a cost-benefit decision that requires honest weight-loss goal-setting, a full review of your medical history, and knowledge of your actual out-of-pocket costs. That is what a telehealth intake is for.
Frequently Asked Questions
Yes, but modestly. The Diabetes Prevention Program found that about 28–30% of participants on metformin lost ≥5% of body weight in the first year, with an average loss of approximately 2.1 kg (roughly 2%) across all participants. Among Year-1 responders, 56.5% maintained ≥5% weight loss across a 14-year follow-up. Metformin works best as a weight-loss adjunct for patients with prediabetes, insulin resistance, or PCOS — it is not an effective standalone weight-loss drug for patients without underlying metabolic dysfunction. Per WebMD’s summary of DPP data, the average long-term loss is approximately 5.5 pounds across the study population. The FDA has not approved metformin for weight loss, and off-label use should be supervised by a licensed provider.
For significant weight loss, yes, by a substantial margin. The SUSTAIN trial program demonstrated 6–9% body weight loss with semaglutide 1.0 mg in type 2 diabetic patients, compared to 2–3% averaged across DPP/DPPOS participants on metformin. Ozempic at 1.0 mg produces approximately three to four times more weight loss on average. However, both drugs are off-label for pure weight loss, the FDA-approved weight-management indication for semaglutide belongs to Wegovy at 2.4 mg, which produced 14.9% weight loss in STEP 1. If cost is a primary constraint and the goal is modest loss, metformin’s $4–$20/month price point versus Ozempic’s $349/month makes metformin the more pragmatic choice for some patients.
Generic metformin costs $4–$20/month with a GoodRx discount, per GoodRx’s April 2026 pricing data. Ozempic’s list price is $1,028/month, but self-pay patients can access it through NovoCare Pharmacy for $199/month for the first two fills (new patients, through June 30, 2026), then $349/month for ongoing 0.5–1.0 mg doses, or $499/month for the 2.0 mg dose. With commercial insurance covering Ozempic for type 2 diabetes, out-of-pocket costs can drop to as little as $25/month via the Ozempic savings card, but off-label weight-loss prescriptions typically do not qualify. The monthly cost gap between the two drugs is $330–$480 for most self-pay patients.
Yes, and this combination has evidence supporting additive benefit. A 2024 meta-analysis (PMC11384358) found that semaglutide combined with metformin significantly reduced BMI versus metformin alone across 10 RCTs. SUSTAIN-7 participants were on background metformin therapy, demonstrating the combination’s real-world effectiveness. The combination is common in clinical practice for type 2 diabetes management and is often appropriate for patients with high BMI who need both glycemic control and meaningful weight loss. Before combining the two, a provider should review your renal function (metformin requires monitoring at reduced eGFR), thyroid history, and GI tolerability, which is part of the standard telehealth intake at WeightLossInjections.com.
The process involves an asynchronous or synchronous consultation with a licensed prescriber who reviews your medical history, BMI, and goals. Because Ozempic’s FDA indication is for type 2 diabetes, a provider prescribing it off-label for weight loss must document clinical rationale. At WeightLossInjections.com, the intake takes under 3 minutes; a licensed provider reviews your submission within 24 hours and, if appropriate, sends a prescription to NovoCare or another pharmacy. If you are a better candidate for Wegovy (the FDA-indicated weight-management semaglutide), or for a GLP-1/GIP dual agonist like tirzepatide, the provider will recommend the appropriate option as part of the consultation. Note that since the FDA declared the semaglutide shortage resolved on February 21, 2025, only brand-name Ozempic and Wegovy, not compounded semaglutide, are available through legitimate telehealth platforms. [Start your free intake →]
This article is for educational purposes only and is not a substitute for professional medical advice. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. All pricing is verified as of April 2026 and is subject to change by manufacturers and pharmacies at any time. Both metformin and Ozempic/semaglutide are used off-label for weight loss; consult a licensed provider to discuss your individual medical history, risk factors, and treatment goals before starting either medication.
![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/04/hero_ozempic_c4_compare-1200x675.png)