![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/05/hero_zepbound_c4_compare-1200x675.png)
SURMOUNT-5 Head-to-Head Weight Loss Results
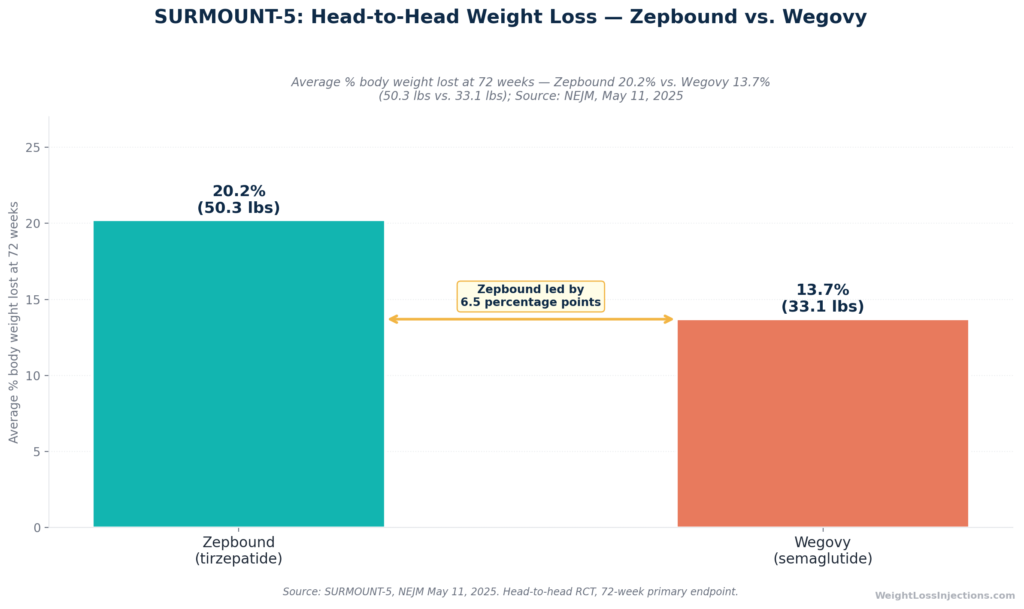
Zepbound (tirzepatide) and Wegovy (semaglutide) are the two FDA-approved weekly injections for chronic weight management in adults. In the only direct head-to-head trial, SURMOUNT-5, published in the New England Journal of Medicine, Zepbound produced 20.2% mean weight loss versus 13.7% for Wegovy at 72 weeks, a 47% greater relative advantage.
But the better drug for you depends on more than a single trial: Wegovy holds FDA approvals for cardiovascular risk reduction and MASH that Zepbound does not, while Zepbound is the only medication approved for obstructive sleep apnea (OSA). Pricing has also shifted dramatically, Zepbound runs $299–$449/mo for self-pay patients via LillyDirect, Wegovy’s injection is $349/mo via NovoCare, and Wegovy’s new oral pill starts at $149/mo.
The Drugs at a Glance
Zepbound and Wegovy look similar on the surface, both are once-weekly injections, both suppress appetite through incretin pathways, and both carry the same FDA indication for chronic weight management. The differences begin at the molecular level and ripple outward into clinical outcomes, approved indications, pricing, and patient selection.
Key Facts Comparison Table
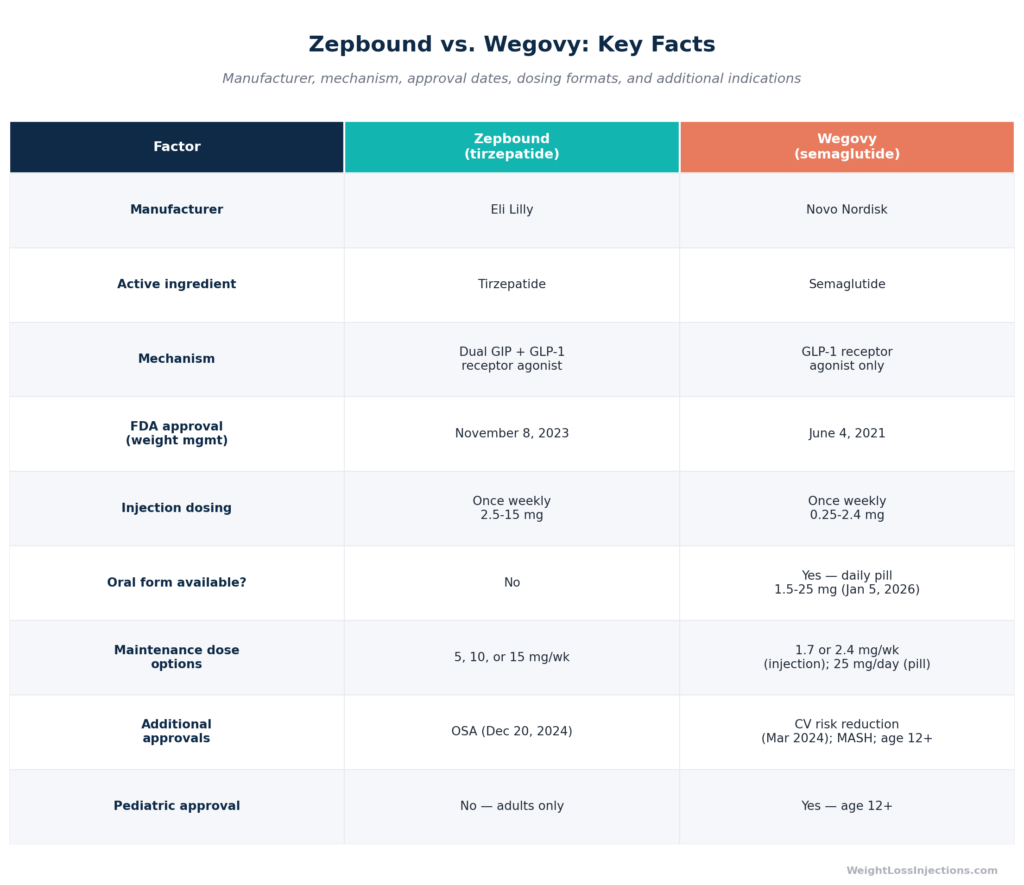
| Factor | Zepbound (tirzepatide) | Wegovy (semaglutide) |
|---|---|---|
| Manufacturer | Eli Lilly | Novo Nordisk |
| Active ingredient | Tirzepatide | Semaglutide |
| Mechanism | Dual GIP + GLP-1 agonist | GLP-1 agonist only |
| FDA weight management approval | November 8, 2023 | June 4, 2021 |
| Injection dosing | Once weekly, 2.5–15 mg | Once weekly, 0.25–2.4 mg |
| Oral form | No | Yes (daily pill, launched Jan 5, 2026) |
| Additional approvals | OSA (Dec 2024) | CV risk reduction; MASH; ages 12+ |
Sources: Zepbound FDA prescribing information; FDA Zepbound approval press release.
How Zepbound and Wegovy Work Differently
Zepbound: Dual GIP + GLP-1 Action
Tirzepatide, the active ingredient in Zepbound, is the first FDA-approved dual GIP receptor (GIPR) and GLP-1 receptor (GLP-1R) agonist, per the Zepbound prescribing information. That two-receptor mechanism is the core reason Zepbound outperforms semaglutide in head-to-head data.
Here is what each receptor does in practice:
- GLP-1 receptor activation slows gastric emptying, reduces appetite via central hypothalamic signaling, and stimulates glucose-dependent insulin secretion. This is the pathway shared with Wegovy.
- GIP receptor activation enhances insulin secretion in a glucose-dependent manner, suppresses glucagon, and has direct effects on adipose tissue — including reducing adipogenesis. These are mechanisms that GLP-1 agonism alone cannot replicate.
The dual-pathway design means tirzepatide can achieve greater appetite suppression and metabolic effects at equivalent tolerability. The proposed mechanism for its superior weight loss is not simply “more GLP-1” but a qualitatively different hormonal signal that activates a broader downstream response, per the Zepbound prescribing information.
Wegovy: The Proven GLP-1 Track Record
Semaglutide, sold as Wegovy for weight management and Ozempic for type 2 diabetes, is a mono GLP-1 receptor agonist. It has been in active clinical use since 2017 (as Ozempic for T2D) and has a longer real-world safety dataset than any other GLP-1 agent used for weight management.
Wegovy’s singular advantage at the pharmacological level is its longer clinical history. It was FDA-approved for weight management on June 4, 2021, more than two years before Zepbound, and the SELECT cardiovascular outcomes trial enrolled over 17,000 patients to demonstrate a reduction in MACE (major adverse cardiovascular events) in patients with established cardiovascular disease. That trial underpins Wegovy’s March 2024 FDA indication for cardiovascular risk reduction, a label Zepbound does not hold.
Head-to-Head Efficacy: What SURMOUNT-5 Shows
The Only Direct Comparison
Until 2025, comparisons between Zepbound and Wegovy were indirect, drawing on SURMOUNT-1 and STEP-1 trials run in different populations, at different time points, with different inclusion criteria. That changed when Eli Lilly published the SURMOUNT-5 results in the New England Journal of Medicine on May 11, 2025.
Trial design: Phase 3b, open-label, randomized; 751 adults with obesity (no type 2 diabetes); 72 weeks; 32 U.S. and Puerto Rico sites. Participants were randomized to tirzepatide at maximum tolerated dose (10 or 15 mg) or semaglutide at maximum tolerated dose (1.7 or 2.4 mg). The open-label design was necessary because pen devices differ, but it is a limitation, participants knew which drug they were taking, per the Eli Lilly SURMOUNT-5 press release.
Primary result: Mean body weight reduction of −20.2% for tirzepatide versus −13.7% for semaglutide at 72 weeks (p<0.001). That is a 47% greater relative weight loss advantage for Zepbound, per PubMed SURMOUNT-5.
In absolute terms, participants taking tirzepatide lost an average of 50.3 lbs (22.8 kg) versus 33.1 lbs (15.0 kg) for semaglutide, a gap of 17 lbs on the same trial timeline, per the Eli Lilly SURMOUNT-5 press release.
Secondary Endpoints
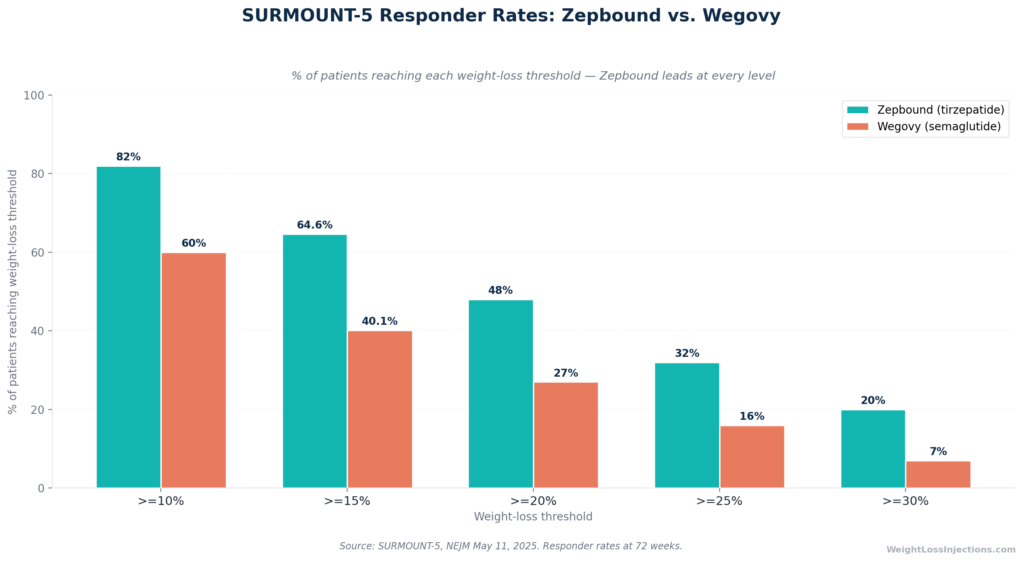
The secondary data from SURMOUNT-5 reinforces the primary finding across every threshold:
| Responder Threshold | Zepbound | Wegovy |
|---|---|---|
| ≥10% body weight lost | 82% | 60% |
| ≥15% body weight lost | 64.6% | 40.1% |
| ≥20% body weight lost | 48% | 27% |
| ≥25% body weight lost | 32% | 16% |
| ≥30% body weight lost | 20% | 7% |
Source: SURMOUNT-5, NEJM May 2025.
Waist circumference reduction also favored tirzepatide: −18.4 cm versus −13.0 cm. Discontinuation due to adverse events was 6.1% for tirzepatide versus 8.0% for semaglutide — numerically lower for Zepbound, though the trial was not powered to formally compare tolerability, per PubMed SURMOUNT-5.
SURMOUNT-5 Responder Rate Chart
The Pivotal Trials in Context
Comparing SURMOUNT-1 (tirzepatide) and STEP-1 (semaglutide) directly is tempting but scientifically problematic — different populations, different placebo-response rates, and different calendar years mean the numbers are not interchangeable. The key figures for context:
- SURMOUNT-1 (tirzepatide 15 mg, 72 weeks, no T2D): −20.9% average weight loss, per NEJM 2022, Jastreboff et al..
- STEP-1 (semaglutide 2.4 mg, 68 weeks, no T2D): −14.9% average weight loss. The design differences — including a shorter primary endpoint at 68 vs. 72 weeks — make these figures unsuitable for direct comparison without the randomization SURMOUNT-5 provided.
A real-world confirmation comes from a JAMA Internal Medicine retrospective analysis of 18,386 matched pairs, which found tirzepatide produced −15.3% versus semaglutide −8.3% weight loss at 12 months. The real-world gap mirrors the trial gap, lending credibility to SURMOUNT-5’s direction of effect.
FDA Approvals: More Than Weight Loss
This is where the two drugs diverge most meaningfully for clinical decision-making. Both are approved for the same core weight management indication, but their secondary approvals point to very different patient populations.
Zepbound’s Additional Indication: Obstructive Sleep Apnea
On December 20, 2024, the FDA approved Zepbound as the first and only prescription medication for moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity, per the Eli Lilly OSA approval press release.
The SURMOUNT-OSA trial data underpinning this approval showed an AHI (apnea-hypopnea index) reduction of −25.3 events per hour with tirzepatide versus −5.3 with placebo in the no-PAP-therapy arm. Forty-two percent of tirzepatide patients in that arm no longer had moderate-to-severe OSA at 52 weeks, compared to 16% on placebo, per the Eli Lilly OSA press release.
This approval has a practical coverage implication: Medicare Part D plans may cover Zepbound when it is prescribed specifically for OSA, a coverage pathway that does not exist for Zepbound prescribed solely for weight management.
Wegovy’s Additional Indications: Cardiovascular, MASH, and Pediatric
Wegovy holds three additional FDA approvals that Zepbound does not:
- Cardiovascular risk reduction (March 8, 2024): Wegovy is the only GLP-1 agent approved to reduce the risk of serious cardiovascular events (cardiovascular death, heart attack, or stroke) in adults with established cardiovascular disease and either obesity or overweight. This approval is grounded in the SELECT trial outcomes data.
- MASH (metabolic dysfunction-associated steatohepatitis with liver scarring): Wegovy 2.4 mg injection is approved for this indication — a meaningful differentiator for patients with liver disease complicating their obesity.
- Pediatric obesity (ages 12 and older): Wegovy is approved for adolescents aged 12 and up. Zepbound is approved for adults only.
Indication Decision Matrix
| Clinical situation | Stronger choice |
|---|---|
| Primary goal: maximum weight loss, no special comorbidities | Zepbound (SURMOUNT-5 data) |
| Moderate-to-severe OSA + obesity | Zepbound (only approved medication) |
| Established cardiovascular disease | Wegovy (FDA CV risk reduction indication) |
| MASH (liver scarring) | Wegovy (approved indication) |
| Patient age 12–17 | Wegovy (Zepbound is adults only) |
| Needle aversion | Wegovy (oral pill option available) |
| Self-pay, lowest cost injection | Zepbound via LillyDirect ($299–$449/mo) |
Side Effects: Which Is Better Tolerated?
Both medications produce gastrointestinal side effects, nausea, diarrhea, vomiting, and constipation, that are characteristic of the GLP-1 incretin class. The frequency differs between the two drugs at their respective highest approved doses.
GI Side Effect Comparison (From FDA Labels, Highest Approved Doses)
| Side Effect | Zepbound 15 mg | Wegovy 2.4 mg |
|---|---|---|
| Nausea | 28% | 44% |
| Diarrhea | 23% | 30% |
| Vomiting | 13% | 24% |
| Constipation | 11% | 24% |
| Abdominal pain | ~10% | ~20% |
Source: Zepbound prescribing information; Green Relief Health head-to-head data summary.
At face value, Zepbound produces lower rates of every GI adverse event at its highest dose compared to Wegovy’s highest dose. This aligns directionally with SURMOUNT-5’s observation that tirzepatide’s discontinuation rate due to adverse events was 6.1% versus 8.0% for semaglutide, per PubMed SURMOUNT-5. However, important caveats apply: these figures come from separate trials with different populations; SURMOUNT-5 was not powered to formally compare tolerability; and 15 mg tirzepatide and 2.4 mg semaglutide are not dose-equivalent (they act on different receptors at different concentrations). Use the table as directional guidance, not a definitive tolerability verdict.
Both drugs produce GI side effects most prominently during dose escalation. Symptoms typically diminish once a stable maintenance dose is established.
Shared Serious Risks
Both Zepbound and Wegovy carry a black box warning for thyroid C-cell tumors based on rodent data. The FDA’s label states the human relevance is unknown, and both drugs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), per the Zepbound prescribing information.
Additional serious risks shared by both agents include:
- Pancreatitis — discontinue if suspected; not studied in patients with a history of pancreatitis
- Gallbladder disease — cholelithiasis and cholecystitis are reported with GLP-1 agents
- Acute kidney injury — from dehydration secondary to nausea, vomiting, and diarrhea
- Hypoglycemia — risk substantially elevated when combined with insulin or sulfonylureas
Per the FDA Zepbound approval press release, neither drug should be combined with the other, nor with any other GLP-1 receptor agonist.
Zepbound-Specific Considerations
The Zepbound label carries specific guidance for patients using oral contraceptives: use backup or alternative contraception for 4 weeks after initiating Zepbound and 4 weeks after each dose escalation, because delayed gastric emptying may reduce oral drug absorption, per the Zepbound prescribing information. This applies to any oral medication with absorption that can be affected by gastric motility.
Wegovy-Specific Considerations
Wegovy’s cardiovascular indication is medically significant for patients with established heart disease who are choosing between these two agents. The SELECT trial’s cardiovascular outcomes data provides safety reassurance in a high-risk population that Zepbound has not yet been specifically evaluated in for MACE outcomes.
Dosing Schedules: Step-by-Step Comparison
Both drugs use a gradual titration designed to minimize GI side effects as the body adjusts. Zepbound has more dose steps, providing finer tolerability control.
| Titration Step | Zepbound | Wegovy Injection | Wegovy Oral Pill |
|---|---|---|---|
| Starting dose | 2.5 mg/wk × 4 wks | 0.25 mg/wk × 4 wks | 1.5 mg/day × 30 days |
| Step 2 | 5 mg/wk × ≥4 wks | 0.5 mg/wk × 4 wks | 4 mg/day × 30 days |
| Step 3 | 7.5 mg/wk × ≥4 wks | 1 mg/wk × 4 wks | 9 mg/day × 30 days |
| Step 4 | 10 mg/wk × ≥4 wks | 1.7 mg/wk × 4 wks | 25 mg/day (maintenance) |
| Step 5 | 12.5 mg/wk × ≥4 wks | 2.4 mg/wk (maintenance) | — |
| Maximum dose | 15 mg/wk | 2.4 mg/wk | 25 mg/day |
Sources: Zepbound prescribing information; GoodRx Zepbound vs. Wegovy dosing comparison.
Zepbound’s titration offers six dose levels versus Wegovy injection’s five, which can make a practical difference for patients who tolerate intermediate dose steps poorly. Both drugs can have their titration slowed at the prescriber’s discretion if GI side effects are problematic.
Wegovy’s oral pill (launched January 5, 2026) uses a four-step daily titration that tops out at 25 mg/day maintenance. The oral format offers an option for needle-averse patients, but long-term efficacy data for the oral form is less extensive than for the injection.
Our Top 3 · August 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
Formats: Injection vs. Pill
Zepbound — Injection Only
As of April 2026, Zepbound is available only as a subcutaneous injection in three formats:
- Single-dose auto-injector pen — prefilled, color-coded by dose, one pen = one weekly dose; available in all six strengths (2.5–15 mg).
- Single-dose vial — requires a separate syringe; all six strengths available; the format sold via LillyDirect at the lowest self-pay prices.
- Multi-dose KwikPen — launched February 23, 2026; four weekly doses per pen; available through LillyDirect for self-pay patients, per CNBC Feb 23, 2026.
No oral tirzepatide formulation has been announced or FDA-approved as of April 2026.
Wegovy — Injection + Oral Pill
Wegovy is available in two formats as of 2026:
- Weekly injection pen — prefilled auto-injector; 0.25 mg to 2.4 mg; the primary clinical data form.
- Oral Wegovy pill — launched January 5, 2026; daily dosing from 1.5 mg starter up to 25 mg maintenance; available through NovoCare Pharmacy. The oral form is a genuine differentiator for patients who are averse to self-injection.
For patients comparing the two drugs, the oral option may be Wegovy’s most practically relevant advantage if needle aversion is a barrier to adherence.
Cost in 2026: The Complete Pricing Picture
Pricing for both medications has changed significantly in the past 12 months. The self-pay options are now meaningfully accessible, and a new Medicare coverage bridge program opens in July 2026.

2026 Pricing Comparison Table
List Prices (WAC)
At wholesale acquisition cost, Zepbound is $1,086/mo for a 28-day supply in any pen strength. Wegovy is approximately $1,349/mo, per verified pricing as of April 2026. Neither figure is what most patients actually pay.
Self-Pay Programs
Zepbound via LillyDirect (Self Pay Journey Program, effective December 1, 2025):
- 2.5 mg: $299/mo
- 5 mg: $399/mo
- 7.5 mg, 10 mg, 12.5 mg, or 15 mg: $449/mo each
These prices apply to single-dose vials and to the new KwikPen through LillyDirect only. Enrollment in the Self Pay Journey Program is required. Without enrollment, LillyDirect prices are higher, per CNBC Dec 1, 2025.
Wegovy via NovoCare Pharmacy:
- Injection pen (all maintenance doses 1 mg–2.4 mg): $349/mo
- Injection pen (starter doses 0.25 mg and 0.5 mg): $199/mo
- Oral Wegovy pill (1.5 mg and 4 mg): $149/mo
- Oral Wegovy pill (9 mg and 25 mg): $299/mo
- 12-month subscription program (launched March 31, 2026): $249/mo for injection or pill, per the Novo Nordisk subscription launch press release
For a self-pay patient comparing injection-to-injection at maintenance doses, Zepbound at $449/mo (LillyDirect, 7.5–15 mg) is more expensive than Wegovy at $349/mo (NovoCare injection) but delivers meaningfully greater average weight loss per SURMOUNT-5. On a cost-per-pound-lost basis, the calculus favors Zepbound for most patients at those doses.
Wegovy’s oral pill at $149–$299/mo is the lowest-priced self-pay option across both brands at maintenance doses, but only if the patient is comfortable with daily dosing and if long-term efficacy data for the oral form, which is still early, holds up.
Commercial Insurance + Savings Cards
With commercial insurance coverage and a manufacturer savings card, both drugs are available for as low as $25/mo, per verified April 2026 program terms. Approximately 43–45% of commercial plans cover Zepbound for weight management; similar coverage rates apply to Wegovy with appropriate diagnosis codes, per Pandameds insurance coverage analysis.
Medicare Coverage
Standard Medicare Part D does not cover either drug for the weight management indication, Medicare is statutorily prohibited from covering drugs used solely for weight loss, per American College of Gastroenterology guidance from April 2025.
Important exceptions:
- Wegovy for cardiovascular indication: Medicare Part D plans may cover Wegovy when prescribed for its cardiovascular risk reduction indication, currently the only standard Medicare Part D pathway available for either drug in a weight-loss context.
- Zepbound for OSA: Medicare Part D plans may cover Zepbound when prescribed specifically for moderate-to-severe OSA, subject to individual plan formulary decisions.
- Medicare GLP-1 Bridge (July 1–December 31, 2026): CMS announced a temporary bridge program providing both Zepbound and Wegovy at a $50 copayment for eligible Medicare Part D enrollees (BMI ≥35, or ≥27 with clinical criteria). This program operates outside the standard Part D benefit and bridges to the longer-term BALANCE Model demonstration beginning in 2027, per KFF analysis from March 2026.
Pricing Summary
| Scenario | Zepbound | Wegovy |
|---|---|---|
| WAC list price | $1,086/mo | $1,349/mo |
| Self-pay (lowest starter dose) | $299/mo (2.5 mg vial, LillyDirect) | $149/mo (oral 1.5 mg, NovoCare) |
| Self-pay (maintenance) | $449/mo (7.5–15 mg, LillyDirect) | $349/mo (injection) or $299/mo (oral 9/25 mg) |
| Commercial insurance + savings card | As low as $25/mo | As low as $25/mo |
| Medicare Bridge (Jul–Dec 2026) | $50 copay | $50 copay |
| Needle-free option? | No | Yes ($149–$299/mo oral) |
Sources: CNBC Dec 1, 2025; Novo Nordisk subscription launch press release; KFF Medicare GLP-1 Bridge analysis.
Switching Between Zepbound and Wegovy
Switching is medically feasible, and many patients do switch, either because of tolerability issues, insurance coverage changes, cost, or clinical reasons. The key rules:
Switching from Wegovy to Zepbound: The general clinical approach is to administer Zepbound’s 2.5 mg starting dose approximately one week after the last Wegovy injection dose, then re-titrate according to the standard Zepbound schedule. Re-titrating from the beginning, rather than starting at a “matching” dose, allows the GI system to adjust to the different receptor engagement profile. Discuss timing with your prescriber.
Switching from Zepbound to Wegovy: Similarly, start Wegovy’s 0.25 mg initiation dose one week after the last Zepbound dose and titrate normally. Do not attempt to dose-match directly.
Critical rule: These drugs must never be taken simultaneously. Tirzepatide activates the GLP-1 receptor, the same receptor semaglutide targets. Combining them creates compounding receptor activation with unpredictable and potentially dangerous consequences, per the FDA Zepbound approval press release. This also applies to any other GLP-1 receptor agonist (liraglutide, dulaglutide, exenatide).
Patients switching for insurance reasons should be aware that each drug requires its own prior authorization process. A prior auth for Wegovy does not automatically transfer to Zepbound, and starting the insurance process before the switch date is advisable.
Contraindications: Who Should Not Take Either Drug
Both Zepbound and Wegovy share the following absolute contraindications:
- Personal or family history of medullary thyroid carcinoma (MTC), both carry a black box thyroid C-cell tumor warning based on rodent studies; human relevance is unknown but the FDA regards the risk as serious enough to contraindicate in MTC history, per the Zepbound prescribing information
- Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
- Known serious hypersensitivity to the active ingredient or any excipient
- Pregnancy — both drugs may cause fetal harm; advise patients to discontinue when pregnancy is recognized
- Concurrent use with each other or with any other GLP-1 agonist
Neither drug has been studied in patients with a prior history of pancreatitis, prescribers should exercise caution and have a documented discussion of risk.
Which Should You Choose? A Decision Guide
The head-to-head data from SURMOUNT-5 establishes Zepbound’s superiority on the primary weight loss endpoint. But the right choice depends on your individual medical profile, insurance situation, and format preferences.
Choose Zepbound If:
- Your primary goal is maximum weight loss and you have no disqualifying comorbidities — SURMOUNT-5 showed a 47% relative advantage for tirzepatide, per PubMed SURMOUNT-5
- You have moderate-to-severe obstructive sleep apnea with obesity — Zepbound is the only FDA-approved medication for this indication, per the Eli Lilly OSA approval press release
- You are a self-pay patient who prefers the injection format and wants the lower-cost option — Zepbound via LillyDirect ($299–$449/mo) is cheaper than the Wegovy injection via NovoCare ($349/mo at maintenance), per CNBC Dec 1, 2025
- You also have type 2 diabetes — Mounjaro (the same molecule, tirzepatide) is available and may be covered under your T2D benefit even if Zepbound is not covered under your obesity benefit
Choose Wegovy If:
- You have established cardiovascular disease — Wegovy’s March 2024 FDA indication for cardiovascular risk reduction and the SELECT trial outcomes data make it the evidence-backed choice for this patient population
- You prefer or require a non-injection format — Wegovy’s oral pill (launched January 5, 2026) is available at $149–$299/mo via NovoCare, with no Zepbound oral equivalent
- You are age 12–17 with obesity — Wegovy is approved for adolescents; Zepbound is adults only
- You have MASH (metabolic dysfunction-associated steatohepatitis with liver scarring) — Wegovy holds an FDA approval for this indication; Zepbound does not
- You are a Medicare beneficiary with established cardiovascular disease — Wegovy’s CV indication creates a Part D coverage pathway that Zepbound’s weight management indication alone does not, outside the temporary Bridge program
Neither Drug Is Appropriate If:
- You have a personal or family history of MTC or MEN 2
- You are pregnant or actively trying to become pregnant
- You are currently taking another GLP-1 receptor agonist
- You have a known serious hypersensitivity to either active ingredient
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: For most adults seeking maximum weight loss with no overriding comorbidities, the clinical evidence now clearly favors Zepbound. The SURMOUNT-5 head-to-head trial settled the efficacy question with as rigorous a design as an open-label comparison permits: tirzepatide’s dual GIP/GLP-1 mechanism produces an average of 17 more pounds lost over 72 weeks, with more patients reaching every weight-loss threshold from 10% to 30%. That is a clinically meaningful difference, not a statistical artifact.
That said, “better on average” is not the same as “right for you.” Wegovy’s cardiovascular outcomes data is the most compelling reason to choose semaglutide over tirzepatide for a specific patient, if you have had a heart attack, stroke, or carry a diagnosis of established cardiovascular disease, the SELECT trial gives Wegovy a genuine evidence base that SURMOUNT-5 does not override. Similarly, the oral pill option makes Wegovy meaningfully more accessible for patients who have tried and failed to adhere to weekly injections.
From a cost standpoint, both drugs are now accessible for self-pay patients in a way they were not two years ago. The Medicare GLP-1 Bridge program opening July 2026 is significant news for seniors who have been locked out of coverage.
Our recommendation: talk to a licensed clinician about your full health picture, not just your weight loss goal. The right drug is the one your prescriber can match to your medical history, insurance situation, and realistic adherence profile. If you want to understand which option fits your specific case, [service detail] with WeightLossInjections.com connects you with a licensed clinician for [$X/month] — and they can review your full profile to recommend the appropriate path.
Frequently Asked Questions
In the only direct head-to-head trial to date, SURMOUNT-5, published in the New England Journal of Medicine in May 2025, tirzepatide (Zepbound) produced 20.2% mean weight loss versus 13.7% for semaglutide (Wegovy) at 72 weeks. That is a 47% greater relative advantage, with absolute averages of 50.3 lbs lost for Zepbound versus 33.1 lbs for Wegovy. Responder rates also favored Zepbound at every threshold, 32% versus 16% for patients losing at least 25% of body weight. However, “better” depends on your health profile: Wegovy has additional FDA approvals for cardiovascular risk reduction, MASH, and pediatric obesity that Zepbound does not hold.
Zepbound (tirzepatide) is a dual GIP and GLP-1 receptor agonist, the first FDA-approved drug to activate both incretin receptors simultaneously, per the Zepbound prescribing information. Wegovy (semaglutide) is a mono GLP-1 receptor agonist. The additional GIP receptor pathway in tirzepatide enhances insulin secretion, suppresses glucagon, and reduces adipogenesis through adipose tissue GIPR, effects beyond GLP-1 agonism alone. This dual mechanism is believed to explain tirzepatide’s greater weight-loss efficacy in head-to-head data.
At list price, Zepbound ($1,086/mo) is less expensive than Wegovy ($1,349/mo). For self-pay patients using manufacturer programs, the comparison depends on format: Zepbound vials via LillyDirect run $299–$449/mo; Wegovy injections via NovoCare are $199–$349/mo; Wegovy’s oral pill runs $149–$299/mo through NovoCare. With commercial insurance and a manufacturer savings card, both drop to as low as $25/mo. The Medicare GLP-1 Bridge program (July–December 2026) covers both at a $50 copayment for eligible Part D enrollees, per KFF analysis from March 2026.
Wegovy launched an oral pill on January 5, 2026, a daily tablet available in a 1.5 mg starter dose titrating up to 25 mg maintenance, sold through NovoCare Pharmacy at $149–$299/mo depending on dose strength. Zepbound is injection-only as of April 2026, no oral formulation is approved or has been announced. Wegovy’s oral pill is a meaningful option for needle-averse patients; however, the injection form carries more long-term efficacy data.
Yes, switching is medically feasible. The general approach when switching from Wegovy to Zepbound is to start at Zepbound’s 2.5 mg initiating dose approximately one week after the last Wegovy injection, then re-titrate on the standard Zepbound schedule. Switching from Zepbound to Wegovy follows the same logic in reverse, start at Wegovy’s 0.25 mg initiating dose one week after the last Zepbound dose. These drugs must never be taken simultaneously, as both activate the GLP-1 receptor pathway and combining them is contraindicated, per the FDA Zepbound approval press release. Always coordinate the transition with your prescribing provider.
Standard Medicare Part D does not cover either drug for the weight management indication, Medicare is statutorily prohibited from covering drugs used solely for weight loss, per American College of Gastroenterology guidance from April 2025. Exceptions: Wegovy may be covered under Part D when prescribed for its cardiovascular risk reduction indication; Zepbound may be covered when prescribed for OSA. A temporary Medicare GLP-1 Bridge program provides both drugs at a $50 copayment from July 1 through December 31, 2026, for eligible Part D enrollees (BMI ≥35 or ≥27 with clinical criteria), per KFF analysis from March 2026.
