
Zepbound SURMOUNT-1 Dose-Response Bar Chart
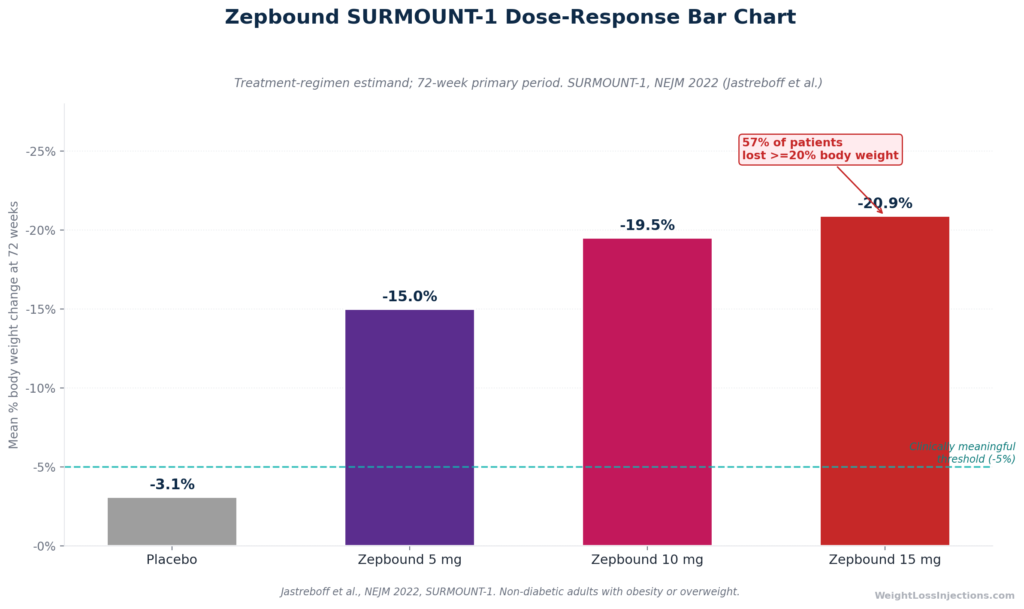
Zepbound doses increase because tirzepatide has a proven, stepwise dose-response: every 2.5 mg step up the titration ladder produces measurably greater weight loss, from −15.0% at 5 mg to −20.9% at 15 mg at 72 weeks in SURMOUNT-1. The minimum interval between steps is 4 weeks, the time needed to reach steady-state plasma concentration.
But escalating to 15 mg is not mandatory; FDA approval explicitly allows maintenance at 5 mg or 10 mg when those doses are working and tolerated.
Why Zepbound Doses Escalate: The Core Clinical Logic
If you’ve just filled your first Zepbound prescription, the titration schedule, six dose strengths over a minimum of 20 weeks, can feel like an unnecessarily slow climb. It isn’t. The structure reflects two pharmacological realities: tirzepatide’s documented dose-response relationship and the time required for GI tissue to adapt to each new drug concentration.
Unlike some medications where a single dose fits most patients, tirzepatide is one of the clearest examples in modern pharmacology of a drug where the dose genuinely matters to the outcome. Higher concentrations activate GIP and GLP-1 receptors more potently, producing stronger satiety signaling, greater appetite suppression, and more profound reductions in energy intake, all of which translate into greater weight loss. That relationship is not theoretical. It is measured across thousands of patients in registered clinical trials.
The starting dose, 2.5 mg, is explicitly described in the Zepbound prescribing information as a tolerability step only, not a therapeutic dose. Meaningful weight reduction begins at 5 mg. From there, the question for every patient and provider is: how high do we need to go, and how fast is it safe to get there?
The SURMOUNT Trials: Quantifying What Each Dose Actually Does
SURMOUNT-1: The Pivotal Data in Non-Diabetic Obesity
Before discussing when and why to escalate, it helps to understand what the clinical trial data actually show at each maintenance dose. SURMOUNT-1 is the foundational reference.
SURMOUNT-1, published in The New England Journal of Medicine in 2022 by Jastreboff et al., enrolled 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, specifically excluding people with type 2 diabetes. The 72-week trial compared three doses of tirzepatide against placebo. Results at 72 weeks (treatment-regimen estimand):
| Group | Mean Body Weight Change | ≥5% Weight Loss | ≥20% Weight Loss |
|---|---|---|---|
| Placebo | −3.1% | 35% | 3% |
| Tirzepatide 5 mg | −15.0% | 85% | — |
| Tirzepatide 10 mg | −19.5% | — | ~45% |
| Tirzepatide 15 mg | −20.9% | 91% | 57% |
Source: SURMOUNT-1 in NEJM 2022; Lilly SURMOUNT-1 press release, June 4, 2022.
The dose-response gradient here is substantial and statistically meaningful at every step. Moving from 5 mg to 10 mg adds approximately 4.5 percentage points of weight loss; moving from 10 mg to 15 mg adds another 1.4 percentage points. The additional benefit narrows toward the top of the titration ladder — but it does not disappear, which is why 15 mg remains a legitimate clinical target for patients who need maximum efficacy and can tolerate it. The placebo-adjusted weight loss at 15 mg was −17.8 percentage points, per the ACC SURMOUNT-1 trial summary.
SURMOUNT-2: The Same Pattern in Type 2 Diabetes
Patients with type 2 diabetes typically lose less weight on GLP-1-class medications — a pattern confirmed in SURMOUNT-2, published in The Lancet in 2023. That trial enrolled 938 adults with BMI ≥27 and T2D over 72 weeks and tested only 10 mg and 15 mg versus placebo. Results:
- 10 mg: −12.8% body weight (vs. −3.2% placebo)
- 15 mg: −14.7% body weight (vs. −3.2% placebo)
The same directional dose-response held: 15 mg outperformed 10 mg by approximately 1.9 percentage points, per the ACC SURMOUNT-2 summary. The glycemic benefits were also dose-dependent: 49% of patients on 15 mg achieved normoglycemic HbA1c below 5.7%, compared to fewer patients at 10 mg, per the same ACC SURMOUNT-2 summary.
How the Titration Ladder Is Structured and Why
Zepbound Titration Timeline
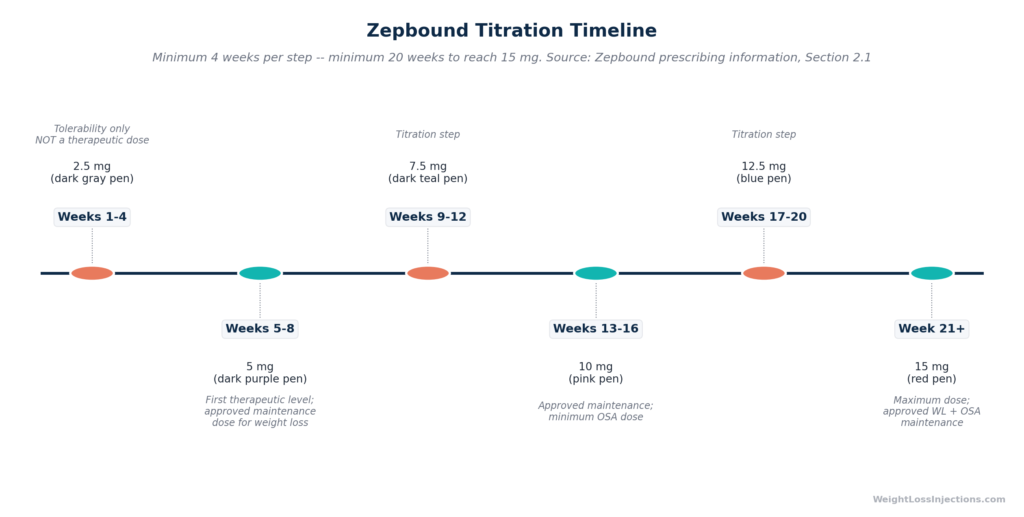
The Zepbound prescribing information, Section 2.1 specifies the following sequence, with each step requiring a minimum of 4 weeks:
| Week Range | Dose | Clinical Purpose | Approved Maintenance Dose? |
|---|---|---|---|
| Weeks 1–4 | 2.5 mg | Tolerability initiation only | No |
| Weeks 5–8 | 5 mg | First therapeutic level | Yes (weight loss) |
| Weeks 9–12 | 7.5 mg | Titration step | No |
| Weeks 13–16 | 10 mg | Optimize dose-response | Yes (weight loss + OSA) |
| Weeks 17–20 | 12.5 mg | Continue titration | No |
| Week 21+ | 15 mg | Maximum dose | Yes (weight loss + OSA) |
Source: Zepbound prescribing information; FDA press release approving Zepbound, November 8, 2023.
Why Exactly 4 Weeks Between Steps?
The 4-week minimum is not arbitrary. Tirzepatide has an elimination half-life of approximately 5 to 6 days, meaning that after starting a new dose, the drug accumulates weekly until steady-state plasma concentrations are reached after approximately 4 weeks of once-weekly dosing, per Zepbound prescribing information.
Escalating faster than every 4 weeks means increasing the dose before the body has had time to reach equilibrium at the current level, the equivalent of turning up the volume before the first song has finished playing. GI side effects typically peak in the first 1 to 2 weeks after a dose increase, then diminish as the GI tract adapts. Rushing the schedule compresses that adaptation window and substantially increases the risk of severe nausea, vomiting, and diarrhea.
Importantly, 4 weeks is a floor, not a ceiling. There is no maximum time a patient can spend at any given dose. A patient who is tolerating 7.5 mg with persistent GI discomfort can stay there for 8, 12, or 20 weeks, whatever it takes for side effects to resolve before advancing.
The Three Approved Maintenance Doses
Among the six dose strengths, only three are FDA-approved as maintenance doses for weight management: 5 mg, 10 mg, and 15 mg. The 7.5 mg and 12.5 mg doses exist solely as titration steps, transition levels the body uses to ramp up. This is a clinically important distinction: a patient who reaches excellent tolerability and adequate weight loss at 7.5 mg should still advance to 10 mg per the prescribing information, unless a specific clinical reason, persistent side effects, goal achieved at 5 mg, argues for stopping short.
Why Your Body Appears to “Need More” Over Time
Patients frequently ask whether Zepbound stops working, whether the drug loses its effect, the way a stimulant might after repeated exposure. The honest clinical answer is more nuanced than a simple yes or no.
Not Tachyphylaxis in the Classical Sense
True tachyphylaxis, receptor desensitization from repeated drug exposure, has not been documented for tirzepatide in peer-reviewed literature. There is no evidence, in the SURMOUNT program or elsewhere, of clinically meaningful GIP or GLP-1 receptor downregulation with sustained tirzepatide use. What has been documented is that tirzepatide’s weight-loss effect continues over time at adequate doses, as shown by the continued weight loss trajectory in SURMOUNT-4’s 36-week open-label lead-in, where patients lost an average of −20.9% over 36 weeks before randomization, per SURMOUNT-4, published in JAMA 2023.
Physiological Adaptation to Weight Loss
What looks like “the drug wearing off” is more accurately explained by the body’s physiological response to weight loss itself. As body weight falls:
- Total daily energy expenditure (TDEE) decreases. A smaller body requires fewer calories to maintain itself. Weight-loss plateaus are partly the result of the body reaching a new caloric equilibrium at lower weight.
- Counter-regulatory hormones activate. Weight loss triggers compensatory increases in ghrelin (the hunger hormone) and reductions in leptin (the satiety hormone), creating a physiological drive to eat more and burn less. This has been documented extensively in the obesity literature and is sometimes described as metabolic adaptation. Research published in Obesity (2016) by Sumithran et al. showed that these hormonal changes persist for at least a year after significant weight loss.
- Relative drug concentration decreases. A patient who has lost 15% of body weight is pharmacologically in a different situation than when they started. The drug concentration per kilogram of body mass may be effectively lower.
These factors, not receptor desensitization, are the primary reason dose escalation can restore weight-loss momentum after a plateau.
What a True Weight-Loss Plateau Looks Like
A clinically meaningful plateau is defined as body weight that has been stable or rising for at least 4 consecutive weeks despite consistent adherence to medication, reduced-calorie diet, and increased physical activity. A single week of stable weight is noise. Four or more weeks of no movement, at a dose level that has not yet produced the target clinical outcome, is a signal worth acting on.
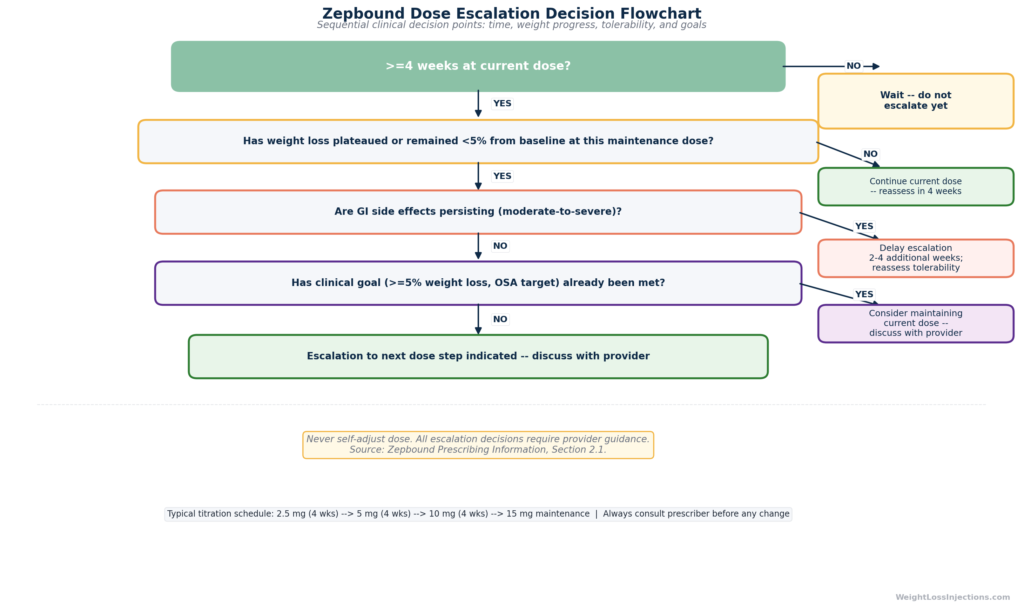
The Zepbound prescribing information frames the minimum efficacy threshold as ≥5% body weight reduction from baseline after an adequate trial at a maintenance dose. If less than 5% has been achieved after ≥12 weeks on a maintenance dose, dose escalation is appropriate.
When Your Provider Will Recommend Escalating
Escalation is typically indicated when all three of the following are true:
- The patient has been at the current dose for at least 4 weeks (steady-state achieved).
- Weight loss has plateaued or total loss from baseline remains below the clinically meaningful threshold of ≥5% of starting body weight.
- The current dose is being tolerated well enough that advancing is unlikely to cause unmanageable GI adverse events.
The FDA-approved Zepbound prescribing information puts escalation decisions squarely in the provider’s hands. Patients should never self-adjust doses, increasing the dose without provider guidance risks severe GI complications and, in patients on insulin or sulfonylurea, acute hypoglycemia.
When to Stay at Your Current Dose (Plateau ≠ Failure)
This is the section most online resources skip. The assumption built into many dose-escalation explanations is that higher is always better, that every patient should be targeting 15 mg as quickly as possible. The FDA label, the SURMOUNT data, and clinical common sense say otherwise.
Legitimate Reasons to Maintain a Lower Dose
Goal met. If a patient at 5 mg has lost 12% of body weight, is tolerating the medication well, and has achieved their clinical targets, blood pressure controlled, A1C normalized, sleep apnea resolved, there is no medical mandate to escalate further. The Zepbound prescribing information explicitly states that 5 mg is an approved maintenance dose for weight management. A patient thriving at 5 mg is not undertreated.
Persistent GI side effects. Moderate-to-severe nausea, vomiting, or diarrhea lasting more than 4 weeks at the current dose is a strong signal to delay escalation. The standard clinical approach is to hold the dose for an additional 2 to 4 weeks until symptoms resolve. Per Zepbound prescribing information, providers may reduce the dose if a maintenance dosage is not tolerated, there is no requirement to push through. Severe GI events causing significant dehydration carry the risk of acute kidney injury, per the same Zepbound prescribing information.
Patient preference. A patient who finds GI side effects at 7.5 mg bothersome but is achieving meaningful weight loss may reasonably prefer to stay at 5 mg rather than advance into a dose range that disrupts daily function. Shared decision-making between patient and provider is the appropriate framework, the label allows it.
Delay vs. Skip: An Important Distinction
Delaying escalation means temporarily staying at the current dose while tolerability issues resolve, then resuming the titration schedule. Skipping a dose step means never advancing to a higher maintenance dose — a legitimate long-term decision when clinical goals are met.
What neither a patient nor a provider should do is increase doses faster than every 4 weeks in an attempt to accelerate results. The titration schedule has hard floors for safety reasons. “Push through early GI side effects at a higher dose” is not a recommended clinical strategy.
The AE Trade-Off: What Happens to Side Effects as Doses Rise
Zepbound GI Adverse Events by Dose
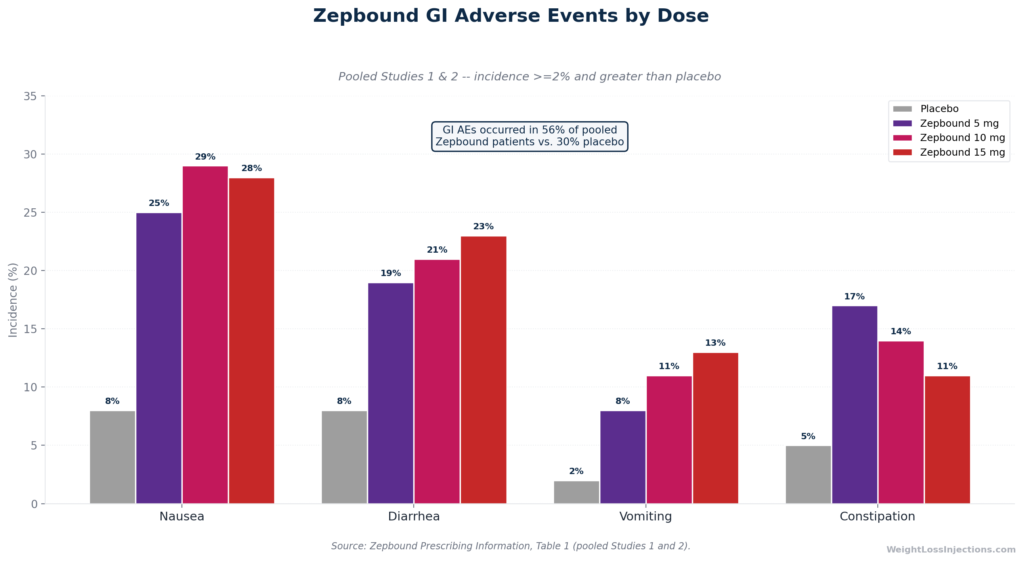
The benefit of dose escalation comes with a clear trade-off: higher doses are associated with higher rates of GI adverse events. The table below summarizes the FDA label data from pooled Studies 1 and 2:
| Adverse Reaction | Placebo | Zepbound 5 mg | Zepbound 10 mg | Zepbound 15 mg |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea† | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation‡ | 5% | 17% | 14% | 11% |
†Includes diarrhea and frequent bowel movements. ‡Includes constipation and feces hard. Source: Zepbound prescribing information, Table 1.
Overall GI adverse reactions occurred in 56% of pooled Zepbound patients versus 30% of patients on placebo, per Zepbound prescribing information. Severe GI events were uncommon but dose-dependent: 1.7% of patients at 5 mg, 2.5% at 10 mg, and 3.1% at 15 mg versus 1.0% on placebo.
Managing Side Effects During Escalation
The first 1 to 2 weeks after any dose increase tend to be the most challenging. Practical mitigation strategies supported by the prescribing information and clinical practice include:
- Reduce meal size. Tirzepatide slows gastric emptying; large meals at a new, higher dose amplify nausea. Per Zepbound prescribing information, patients should avoid high-fat, high-volume foods during the escalation window.
- Stay well hydrated. GI-mediated fluid loss from vomiting or diarrhea can cause dehydration leading to acute kidney injury, per Zepbound prescribing information. Consistent fluid intake is essential.
- Oral contraceptive users: use backup contraception. Gastric emptying delay reduces oral drug absorption. The Zepbound prescribing information requires a backup or non-oral contraceptive method for 4 weeks after each dose escalation (and for 4 weeks after starting Zepbound).
- Patients on insulin or sulfonylureas: discuss dose adjustment. Risk of hypoglycemia increases as Zepbound suppresses appetite and reduces caloric intake. Insulin or sulfonylurea dose reductions should be reviewed with the prescribing provider before escalation, per Zepbound prescribing information.
OSA Patients: A Higher Dose Is Non-Negotiable
Patients using Zepbound for the obstructive sleep apnea indication face a stricter escalation requirement. While weight management patients have three FDA-approved maintenance doses (5 mg, 10 mg, or 15 mg), the Zepbound prescribing information, Section 2.2 specifies that approved maintenance doses for the OSA indication are 10 mg or 15 mg only. The 5 mg dose is not approved for sleep apnea.
This requirement reflects the physiology of the indication. Reducing apnea-hypopnea index (AHI) requires more substantial weight loss, and the higher drug concentrations needed to drive it, than general weight management in some patients. The SURMOUNT-OSA trial (two parallel 52-week Phase 3 RCTs) showed tirzepatide at 10 or 15 mg reduced AHI by 25.3 events per hour (vs. 5.3 events/hour for placebo) in patients not on PAP therapy, per Eli Lilly OSA approval press release. The FDA approved the OSA indication on December 20, 2024, making Zepbound the first and only prescription medication for this use.
If you are prescribed Zepbound for OSA and have been tolerating 5 mg well with good weight loss, your provider will still need to advance you toward 10 mg before establishing a long-term maintenance dose. This is not optional under the current FDA approval.
Does Dose Affect Cost? What Patients Need to Know
One common misconception is that staying at a lower dose is a cost-saving strategy. In most cases, it is not.
For commercially insured patients with Zepbound coverage, the savings card offered by Eli Lilly caps monthly out-of-pocket costs at as low as $25/mo regardless of dose, per Zepbound savings program terms (verified April 2026). The dose you take has no impact on that cost.
For self-pay patients using the LillyDirect Self Pay Journey Program, which offers the lowest available Zepbound prices without insurance, the pricing as of December 1, 2025 is:
| Dose | LillyDirect Self-Pay (Journey Program) |
|---|---|
| 2.5 mg | $299/mo |
| 5 mg | $399/mo |
| 7.5 mg | $449/mo |
| 10 mg | $449/mo |
| 12.5 mg | $449/mo |
| 15 mg | $449/mo |
Source: CNBC, December 1, 2025.
Once a patient moves above 5 mg, all higher doses cost the same $449/mo under the Journey Program. There is no financial incentive to stay at 7.5 mg instead of 10 mg, or at 10 mg instead of 15 mg. The list price at retail pharmacies — $1,086/mo for all dose strengths — is also uniform across doses, per Eli Lilly pricing information (verified April 2026). Clinical factors, not cost, should drive the escalation decision for most patients.
A Patient Framework for Discussing Dose Escalation With Your Provider
The decision to increase, or not increase, your Zepbound dose should be a structured conversation, not a default setting. Here is a practical framework for that discussion.
Zepbound Dose Escalation Decision Flowchart
Questions to bring to your appointment:
- How much weight have I lost from my starting weight so far? Your provider should have a baseline weight on record. Ask for the percentage, not just the number of pounds — it is the clinically relevant figure.
- Am I at a maintenance dose or a titration step? If you are at 7.5 mg or 12.5 mg, you are at an intermediate step with no long-term data behind it. Knowing this helps frame the escalation conversation.
- What GI symptoms should prompt a call before my next appointment? Severe vomiting or diarrhea that is causing you to skip doses or become significantly dehydrated warrants earlier contact.
- What is my target dose based on my indication? If you are on Zepbound for OSA, ask explicitly whether you need to reach 10 mg or 15 mg and what the timeline looks like.
- Is there a clinical reason to stop at a lower dose? If you are doing well at 5 mg or 7.5 mg, ask whether your provider sees value in escalating given your current response.
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: The dose-escalation schedule is one of the most misunderstood aspects of Zepbound therapy, both by patients who want to rush to 15 mg as fast as possible, and by those who resist every increase out of fear of side effects. The SURMOUNT-1 data are clear: every maintenance dose produces meaningful weight loss. The question is not “should I go higher?” but “does the expected additional benefit at a higher dose outweigh the additional GI burden for this specific patient, given their current progress and tolerability?”
That is a question that requires an actual clinical relationship, a provider who knows your response history, your comorbidities, your baseline weight, and your lifestyle. At WeightLossInjections.com, our [service detail] includes provider-supervised titration through every dose step, with structured follow-up at each escalation decision point. Monthly bundled pricing from [$X/month] covers telehealth visits, prescription management, and ongoing clinical oversight, so the dose your body needs is guided by data, not guesswork.
Frequently Asked Questions
Why does my doctor keep increasing my Zepbound dose?
Your doctor is following the FDA-approved titration schedule for Zepbound, which is designed to produce progressively greater weight loss at each step. Each dose increase adds measurable benefit: SURMOUNT-1 showed −15.0% weight loss at 5 mg, −19.5% at 10 mg, and −20.9% at 15 mg over 72 weeks, per SURMOUNT-1 in NEJM 2022. The schedule also allows the GI tract time to adapt at each level before advancing. If weight loss has plateaued and you have not yet reached your clinical goal, escalation is appropriate, but it is always a shared decision between you and your provider.
What happens if I stay at 5 mg Zepbound instead of going higher?
Staying at 5 mg is an FDA-approved option for weight management, and many patients achieve meaningful results at this level. SURMOUNT-1 showed an average of −15.0% body weight reduction at 72 weeks at 5 mg, with 85% of patients losing ≥5% of body weight, per SURMOUNT-1 in NEJM 2022. If your clinical goals are met and you are tolerating the medication well, there is no requirement to escalate. However, the 5 mg dose is not approved for the obstructive sleep apnea indication, OSA patients must reach at least 10 mg, per Zepbound prescribing information.
How long should I stay at each Zepbound dose before increasing?
A minimum of 4 weeks is required between dose increases, this is the time needed for tirzepatide to reach steady-state plasma concentrations after a weekly dosing schedule begins, per Zepbound prescribing information. There is no maximum. If tolerability is a concern, your provider can extend the time at any dose for as long as clinically appropriate before advancing. The 4-week minimum is a safety floor, not an escalation deadline.
Can I skip a dose increase if I’m already losing weight?
Yes, in most cases. The Zepbound prescribing information allows patients to maintain at 5 mg or 10 mg if those doses are meeting their weight management goals. You do not need to reach 15 mg if 5 mg or 10 mg is working. The exception is the OSA indication: patients prescribed Zepbound for sleep apnea must reach at least 10 mg as a minimum maintenance dose, per Zepbound.lilly.com OSA dosing page.
Is the maximum dose of Zepbound (15 mg) always necessary?
No. The Zepbound prescribing information makes clear that 5 mg, 10 mg, and 15 mg are all approved maintenance doses for weight management, and providers should aim for the lowest dose that achieves clinical goals with acceptable tolerability. 15 mg produces the greatest weight loss on average, 57% of SURMOUNT-1 patients on 15 mg lost ≥20% of body weight, per SURMOUNT-1 in NEJM 2022, but it also carries the highest rate of GI adverse events. The right target dose varies by patient.
What does a Zepbound weight-loss plateau mean?
A plateau on Zepbound, defined clinically as stable or rising weight for 4 or more consecutive weeks despite medication adherence, diet, and exercise, can reflect several things: physiological adaptation to weight loss (decreased TDEE, counter-regulatory hormone changes), an underdose relative to the body’s compensatory response, or non-adherence to dietary guidelines. It is not evidence that the drug has stopped working or that receptor desensitization has occurred. Research on weight-loss counter-regulation, including Sumithran et al. in Obesity (2016), shows that hormonal adaptations driving hunger and reduced metabolism can persist for over a year after significant weight loss, which is why dose escalation, when clinically appropriate, can meaningfully restore weight-loss trajectory.