
Zepbound GI Adverse Event Rates by Dose vs. Placebo (Bar Chart)
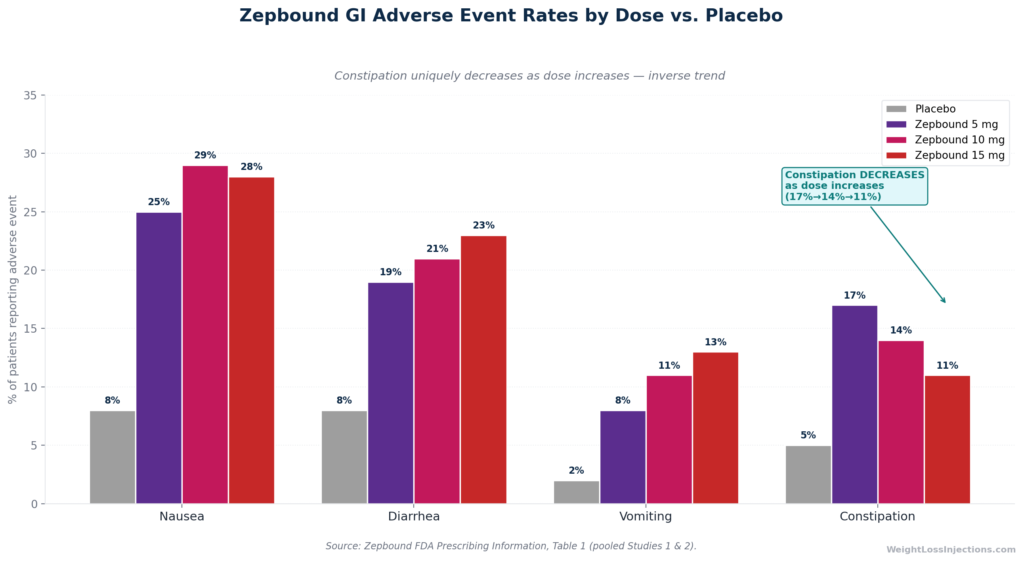
- Constipation is confirmed in Zepbound’s FDA prescribing information, affecting 17% of patients at 5 mg, 14% at 10 mg, and 11% at 15 mg, versus 5% on placebo.
- There is a counterintuitive inverse trend: constipation is highest at the lowest maintenance dose (5 mg) and decreases as the dose goes up, the opposite pattern from nausea and diarrhea.
- Two distinct mechanisms drive it: pharmacological (slowed colonic transit from GLP-1 receptor activation) and nutritional (reduced fiber and fluid intake from eating less).
- Most constipation resolves within 1–3 months at any given dose level as the gut adapts; persistent cases are almost always the nutritional type.
- First-line management is hydration + soluble fiber + daily movement; osmotic laxatives (polyethylene glycol / Miralax) are safe and non-habit-forming for ongoing use.
- Call your provider if you go 3 or more days without a bowel movement, develop abdominal pain or fever, or see blood in stool.
Safety notice: This article is for educational purposes only and does not constitute medical advice. If you are experiencing severe, painful, or persistent constipation on Zepbound, contact your prescribing provider. Abdominal pain accompanied by fever or blood in stool requires urgent evaluation.
Does Zepbound Cause Constipation? The FDA Data
Constipation is among the least-discussed GI side effects of Zepbound, yet for roughly 1 in 7 patients on the 5 mg dose, it is more persistent and disruptive than the more visible complaints of nausea and vomiting. Unlike those symptoms, which tend to announce themselves loudly and resolve relatively quickly, constipation on Zepbound can quietly persist for weeks and worsen if diet isn’t adjusted to compensate.
The answer to whether Zepbound causes constipation is unambiguous. The Zepbound prescribing information, Table 1, which pools data from Studies 1 and 2 of the SURMOUNT clinical program, the trials underlying FDA approval on November 8, 2023, reports constipation (including “feces hard”) at all three maintenance dose levels versus placebo. The numbers are reproduced below directly from the label.
What the Prescribing Information Says
The adverse event data from the Zepbound FDA prescribing information, Table 1, pooling Studies 1 and 2 (N=3,477), shows the following constipation incidence:
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea† | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation‡ | 5% | 17% | 14% | 11% |
†Includes diarrhea and frequent bowel movements. ‡Includes constipation and feces hard.
Source: Zepbound prescribing information, Table 1
Overall GI adverse reactions occurred in 56% of pooled Zepbound patients versus 30% on placebo, confirming that the gastrointestinal tract bears the primary burden of tirzepatide’s side effects, per the Zepbound prescribing information. Severe GI events were uncommon: 1.7% at 5 mg, 2.5% at 10 mg, and 3.1% at 15 mg, compared with 1.0% for placebo.
The Counterintuitive Inverse Dose–Constipation Relationship
The most clinically distinctive feature of the Zepbound constipation data, and the detail that most competing articles miss entirely, is the inverse dose-response trend. Constipation runs at 17% on 5 mg, drops to 14% at 10 mg, and falls further to 11% at 15 mg. This is the precise opposite of what nausea and diarrhea do: both of those increase as the dose goes up.
Why does this matter clinically? It means that dose escalation does not worsen constipation the way it worsens nausea. The 5 mg dose level, weeks 5 through 12 for most patients on the standard titration schedule, is the highest-burden period for constipation. As patients advance through 10 mg and 15 mg, constipation rates actually decline. According to the SURMOUNT-4 trial in JAMA 2023, which included a 36-week open-label lead-in period at maximum maintenance doses (10 or 15 mg), GI adverse events including constipation showed improvement over time as patients reached higher doses and the gut adapted.
This pattern also suggests that the pharmacological mechanism driving constipation is not simply “more drug equals worse gut.” Something more nuanced is happening, and understanding it requires separating the two distinct causes.
Why Does Zepbound Cause Constipation? Two Distinct Mechanisms
Zepbound constipation is not a single phenomenon. It has two mechanistically separate causes, and the distinction matters for treatment because the fix is different for each.
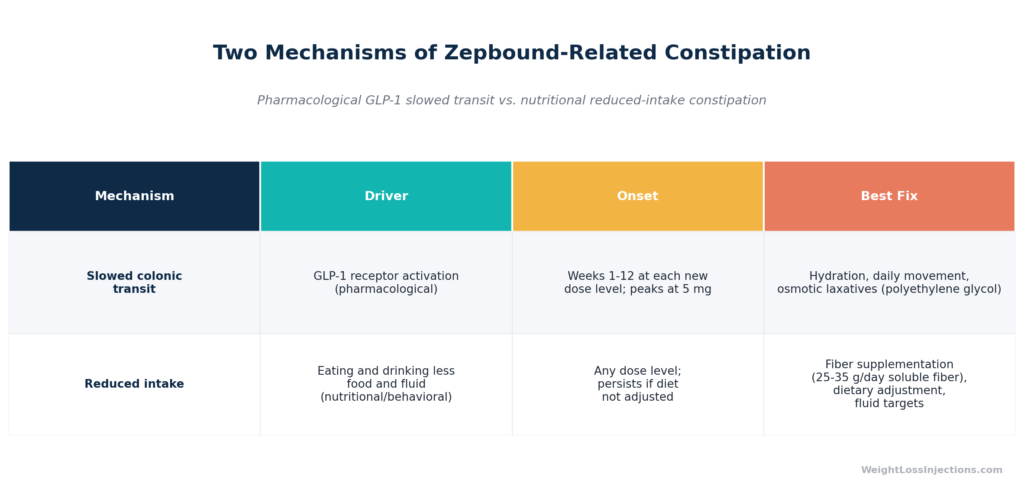
Two Mechanisms of Zepbound-Related Constipation (Comparison Table)
Mechanism 1: Slowed Colonic Transit from GLP-1 Receptor Activation
Tirzepatide is a dual agonist of the GIP receptor (GIPR) and the GLP-1 receptor (GLP-1R), as established in the Zepbound prescribing information and detailed in the FDA pharmacology review for NDA 217806. GLP-1 receptors are distributed throughout the enteric nervous system, not just in the stomach but along the entire intestinal tract, including neurons that regulate colonic motility and transit time.
When tirzepatide activates GLP-1 receptors, it reduces gastric emptying rate. This is the same mechanism that produces nausea, but its downstream effect on the colon is different: slower transit of colonic contents means more time for water to be reabsorbed from the stool, resulting in harder, drier stools that are more difficult to pass. Colonic transit time is prolonged, not just gastric emptying. This is a direct pharmacological effect of the drug, dose-dependent and predictable, and it peaks in the first 4–12 weeks at any given dose level before the gut partially adapts.
The reason constipation is actually worse at 5 mg than at higher doses likely reflects the fact that early-phase GLP-1 receptor engagement has the most dramatic initial effect on colonic motility, and that GIP receptor co-activation at higher doses may partially counterbalance some of the GLP-1-driven slowing, though the precise mechanism of the inverse relationship has not been definitively characterized in published pharmacology literature. The SURMOUNT-1 trial in NEJM 2022 (Jastreboff et al.) confirmed that GI adverse events were concentrated in the early weeks of treatment at each dose level, consistent with a pharmacological adaptation model.
Mechanism 2: Reduced Food and Fluid Intake
The second driver of constipation on Zepbound is not pharmacological at all, it is behavioral and nutritional, and it is the harder one to fix because it persists at any dose until addressed.
Zepbound’s primary mechanism of action is appetite suppression and satiety signaling. In SURMOUNT-1 (Jastreboff et al., NEJM 2022), patients on tirzepatide 15 mg lost an average of 20.9% of body weight over 72 weeks, versus 3.1% on placebo, a reduction that requires sustained decrease in caloric intake. Many Zepbound users, particularly in the first months of treatment, eat 30–50% less food than before. That reduction in food volume directly reduces fiber intake, which is the primary driver of stool bulk and colonic transit regularity. Simultaneously, reduced food intake is often accompanied by reduced fluid intake, either because hunger signals that drive meal-associated drinking are suppressed, or simply because eating less means consuming less fluid from food.
The consequence is predictable: low fiber intake, low fluid intake, and a slower colon equal hard, infrequent stools. This type of constipation does not require dose-dependent timing, it can occur at 5 mg, 10 mg, or 15 mg, and it persists as long as the dietary cause remains uncorrected.
Per the Zepbound prescribing information, Zepbound is indicated as an adjunct to a reduced-calorie diet and increased physical activity, meaning reduced food intake is expected and intentional. Managing the GI consequences of that intake reduction is part of the clinical management plan.
Who Is at Highest Risk?
Based on the FDA label’s dose-stratified data and established gastroenterology risk factors, the patients most likely to experience significant constipation on Zepbound are:
- Patients at the 5 mg dose level — the FDA-label constipation rate of 17% is highest here
- Those who dramatically restrict food volume without compensating with fiber-rich foods or supplements
- Patients with pre-existing constipation or sluggish gut motility
- Those with low baseline physical activity — movement is a major driver of colonic peristalsis
- Patients taking concurrent constipating medications (iron supplements, opioids, certain antihypertensives, calcium channel blockers)
- Older adults, who have slower baseline colonic transit independent of medication
When Does Zepbound Constipation Start, and How Long Does It Last?
Understanding the timeline of constipation on Zepbound requires mapping it to the dosing schedule. Because tirzepatide’s GI effects are dose-level-specific — they peak in the early weeks of each new dose level and then partially resolve as the gut adapts — the constipation arc follows the titration schedule.
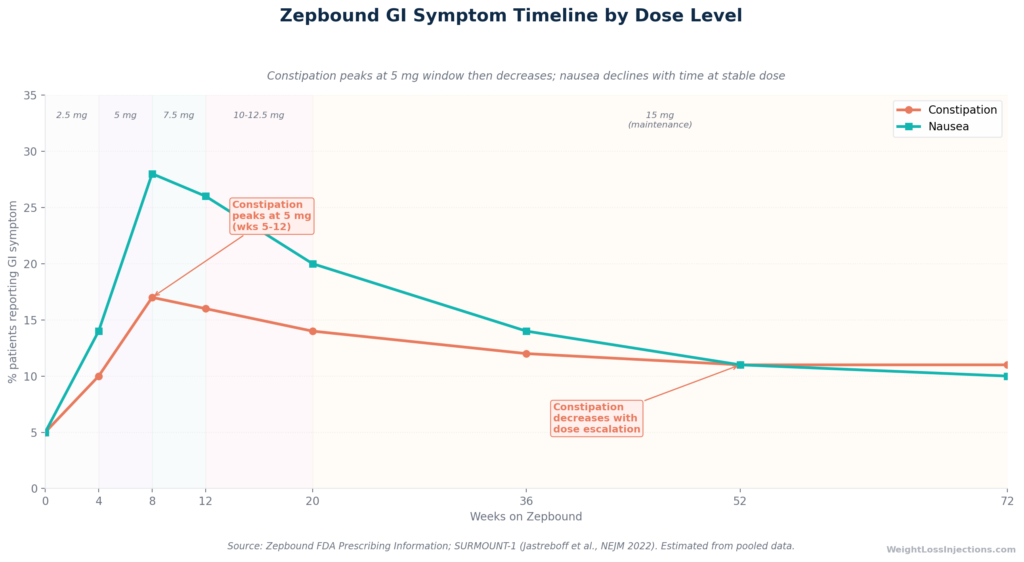
Zepbound GI Symptom Timeline by Dose Level (Line Chart)
Timeline Overview
Weeks 1–4 (2.5 mg starting dose): The 2.5 mg dose is a tolerability step only, not an approved maintenance dose per the Zepbound prescribing information. GI effects at this dose are at their minimum. Most patients experience mild or no constipation during this window, though some report harder stools beginning days 3–7 as gastric emptying slows.
Weeks 5–12 (5 mg dose level): This is the highest-constipation window for most patients. The FDA label’s 17% constipation rate for 5 mg is generated primarily during this period. For patients who also drop their food and fluid intake substantially at the 5 mg level, when appetite suppression becomes pharmacologically significant, the nutritional mechanism kicks in alongside the pharmacological one, compounding the effect.
Weeks 13 onward (escalating through 7.5 mg → 10 mg → 15 mg): Per the SURMOUNT-1 NEJM data (Jastreboff et al., 2022), GI adverse events decline over time at stable doses, and the FDA label’s lower constipation rates at 10 mg (14%) and 15 mg (11%) reflect this improvement. For most patients, constipation is most notable in the 5 mg window and gradually becomes less problematic as they advance through the titration schedule.
Month 3–6 and beyond: As reported in the SURMOUNT-4 trial (JAMA 2023), which tracked patients through a 36-week open-label lead-in at maximum maintenance doses, GI adverse events including constipation were predominantly mild to moderate in severity and improved over the treatment duration. By months 3–6, the majority of patients whose constipation was pharmacological in origin have adapted. Persistent constipation beyond this window almost always has a nutritional cause that needs direct attention.
Does Constipation Go Away?
For most patients: yes, within 1–3 months of any given dose level as the gut adapts to the new colonic transit environment. For a meaningful minority, persistent constipation reflects the nutritional mechanism, inadequate fiber and fluid intake that has not been corrected. This type does not resolve on its own; it requires dietary intervention.
The SURMOUNT-4 JAMA 2023 data are reassuring on the long-term picture: patients who continued tirzepatide through 88 weeks (36-week lead-in plus 52-week double-blind continuation) showed continued weight loss (−25.3% from baseline) with no emerging late GI safety signals, consistent with a medication that is well-tolerated over the long term once the early adaptation period is complete.
How to Relieve Zepbound Constipation: A Step-by-Step Protocol
The following protocol is organized as a sequenced escalation, start with Step 1 and add subsequent steps only if the prior step is insufficient. Most patients resolve their constipation at Step 1 or 2.
Step 1: Hydration, The Most Underestimated Fix
Dehydration is one of the most common and most correctable causes of constipation on Zepbound. When patients eat less, they typically drink less, both because food contributes meaningfully to daily fluid intake (fruits, vegetables, and cooked foods have high water content) and because hunger-associated drinking is suppressed alongside appetite.
The target is 2–3 liters of total fluid daily. Plain water is effective; electrolyte-containing beverages can help patients who are also experiencing GI losses from nausea or diarrhea. The Zepbound prescribing information identifies dehydration from GI adverse reactions as a risk factor for acute kidney injury (AKI), giving hydration a safety rationale that goes beyond bowel health, a point worth taking seriously during the dose-escalation phase.
Practical approach: drink a full glass of water at each meal and between meals, regardless of thirst. Hunger and thirst signals are both suppressed by tirzepatide; patients cannot rely on thirst to guide hydration on this medication.
Step 2: Fiber Optimization
The target fiber intake for adults is 25–35 grams per day per standard dietary guidelines. Most Americans consume roughly 15 grams per day, and Zepbound patients eating reduced food volumes are likely consuming even less. Restoring adequate fiber is essential for stool bulk and colonic transit.
Preferred: soluble fiber. For Zepbound patients, soluble fiber (psyllium husk, chia seeds, oats, flaxseed) is preferred over insoluble fiber as the primary supplement, for two reasons. Soluble fiber absorbs water and forms a gel that softens stool consistency, directly counteracting the dry, hard stools caused by slowed transit. Insoluble fiber (wheat bran, vegetable skins) adds mechanical bulk but can worsen bloating and cramping when transit is already slow. Both types are found in whole foods, but supplemental fiber for Zepbound constipation should prioritize soluble sources.
Introduce gradually. Rapid fiber increases cause gas, bloating, and cramping. Increase fiber intake by no more than 5 grams per week, aiming for 25–35 grams total over 4–6 weeks. This is especially important because Zepbound patients may already be experiencing gas and bloating from altered GI motility.
Critical caveat: Bulk-forming fiber supplements (psyllium in large doses, Metamucil) without adequate fluid intake can worsen constipation and, in rare cases, cause intestinal obstruction. Always increase water intake concurrently with fiber supplementation.
Step 3: Movement
Physical activity directly stimulates colonic peristalsis, the rhythmic muscular contractions that propel stool through the colon. Even modest movement has a measurable effect on colonic transit time. A 20-minute daily walk is enough to make a clinically meaningful difference. This is particularly important for Zepbound users who may reduce activity during the early fatigue phase of treatment, when appetite suppression and caloric restriction create a low-energy period that discourages movement.
Zepbound is FDA-indicated as an adjunct to increased physical activity, so maintaining movement serves both the medication’s therapeutic goal and GI health simultaneously. Daily walks, even short ones, are a simple and zero-cost first-line intervention.
Step 4: OTC Escalation Ladder
When hydration, fiber, and movement are insufficient, over-the-counter laxatives provide the next tier. The following ladder reflects evidence-based gastroenterology guidance for functional constipation and is organized by mechanism:
First-line: Osmotic laxatives (polyethylene glycol, Miralax)
Polyethylene glycol (PEG) works by drawing water into the colon osmotically, softening stool and stimulating passage without being absorbed systemically. It is non-habit-forming and safe for extended daily use in adults, a key advantage for Zepbound patients who may need weeks of support during the 5 mg dose window. Standard adult dosing is 17 grams (one capful) dissolved in 8 oz of liquid once daily. PEG takes 1–3 days to produce a bowel movement from a starting baseline. There are no known pharmacokinetic interactions between PEG and tirzepatide.
Second-line: Stool softeners (docusate sodium, Colace)
Docusate sodium is a surfactant that lowers surface tension in the stool, allowing water to penetrate and soften the stool mass. It is most useful when stool is hard and painful to pass but colonic transit is adequate, making it a complement to PEG rather than a replacement. Standard adult dose: 100–300 mg daily. Docusate is not effective as a standalone agent for severe constipation or when colonic transit is significantly slowed; it works best as an adjunct.
Third-line: Stimulant laxatives (senna, bisacodyl)
Stimulant laxatives directly activate colonic nerve endings to trigger muscular contractions and expel stool. They are effective but should be reserved for situations where the patient has not had a bowel movement in 3 or more days and osmotic agents have not been adequate. Use sparingly, stimulant laxatives can cause cramping, and chronic high-dose use has been associated with dependence effects on colonic motility in some patients, though moderate intermittent use is generally considered safe by gastroenterology consensus.
What Not to Do
- Do not reduce or skip your Zepbound dose to address constipation without consulting your provider. Constipation alone is not a clinical indication to pause tirzepatide. The decision to delay dose escalation or reduce dose involves multiple clinical factors and should not be made unilaterally.
- Do not take bulk-forming fiber supplements without adequate fluid intake. Psyllium and similar products can form a gel mass in the GI tract if taken without sufficient water, potentially worsening constipation or causing obstruction.
- Do not use stimulant laxatives daily as routine maintenance. They are a rescue tool, not a maintenance strategy.
- Do not assume loose stools mean constipation has resolved. Paradoxical diarrhea, liquid stool passing around an impaction — is possible. If loose stools are accompanied by abdominal bloating and the sense of incomplete emptying, contact your provider before treating the loose stools with antidiarrheal medication.
Dose Escalation and Constipation: When to Hold vs. When to Proceed
One of the most clinically relevant questions for Zepbound patients and providers is whether constipation should trigger a delay in dose escalation. The answer, in most cases, is no — but with important exceptions.
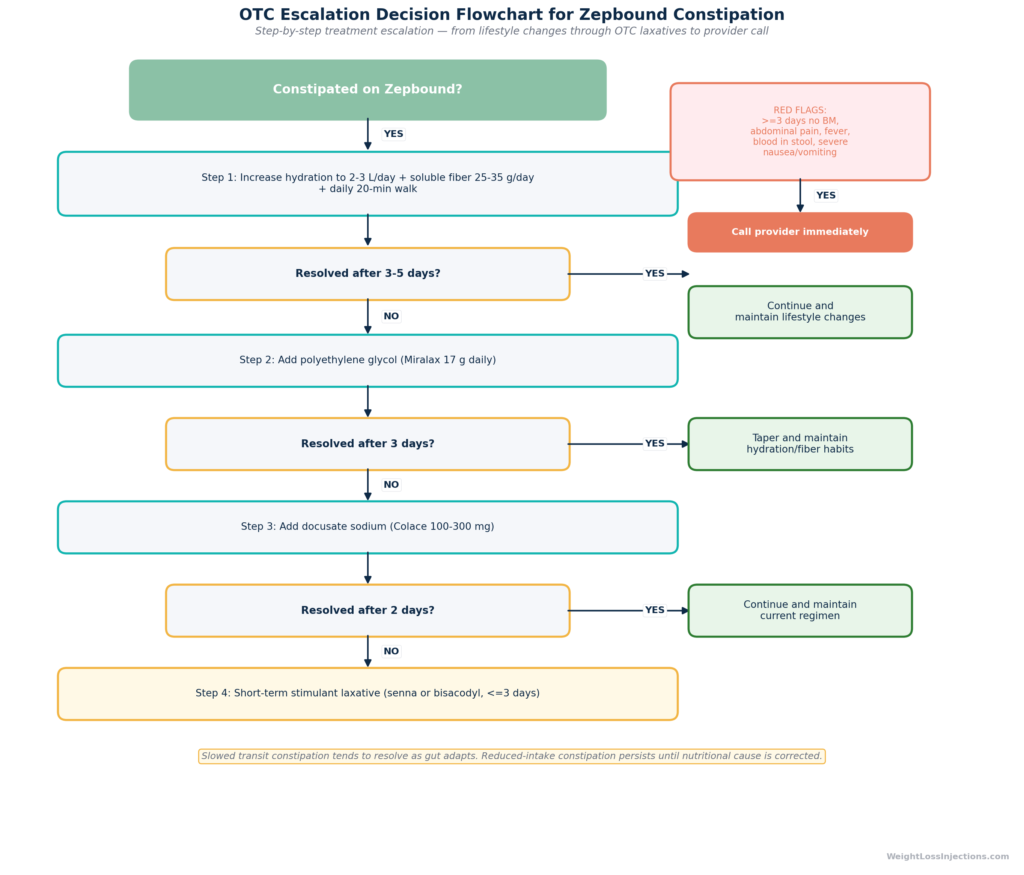
OTC Escalation Decision Flowchart for Zepbound Constipation
When Constipation Alone Does Not Require Holding the Dose
The standard titration schedule, each dose held for a minimum of 4 weeks per the Zepbound prescribing information — is designed with GI tolerance in mind. Mild to moderate constipation without red-flag features (abdominal pain, fever, inability to pass gas, blood in stool) is not, by itself, a clinical reason to delay escalation. Moving to the next dose level often reduces constipation, as the FDA-label data clearly show, rather than worsening it. Holding at 5 mg indefinitely because of constipation may actually prolong the highest-constipation period rather than resolve it.
The SURMOUNT-1 (NEJM 2022) and SURMOUNT-2 (Lancet 2023) trials allowed dose escalation to proceed on schedule in the vast majority of patients despite GI adverse events, confirming that these symptoms, while common, do not routinely require delay.
When to Consider Holding Dose Escalation
Delay escalation and contact your provider if:
- Constipation is accompanied by significant abdominal pain, cramping, or distension — this may indicate a partial obstruction or ileus requiring evaluation
- Constipation is co-occurring with severe nausea and vomiting that prevents adequate fluid intake — the combination creates a dehydration risk that should be addressed before increasing the drug’s GI burden
- There has been no bowel movement in 5 or more days despite OTC management — this warrants provider evaluation before proceeding
Constipation in the context of these warning features is qualitatively different from the typical low-grade delayed transit seen in most patients. It requires clinical assessment, not simply a dose delay.
When to Call Your Doctor About Zepbound Constipation
The following criteria define when constipation on Zepbound moves from a manageable side effect to a situation requiring professional evaluation. Contact your provider promptly if:
- No bowel movement for 3 or more days despite hydration, fiber, and osmotic laxative use
- Abdominal pain that is more than mild — cramping, distension, or pain that does not resolve after a bowel movement
- Fever accompanying constipation — suggests possible infection or serious GI complication
- Blood in the stool — not an expected consequence of tirzepatide; requires investigation to rule out other causes
- Severe nausea or vomiting combined with constipation — the combination creates risk for dehydration and acute kidney injury, per the Zepbound prescribing information’s AKI precaution
- Constipation that significantly impairs your quality of life at a given dose level for more than 4 weeks without improvement — this is a conversation to have about management options, which may include an extended hold at the current dose or review of dietary factors
The 3-day threshold for no bowel movement (without resolution by OTC means) is consistent with current gastroenterology guidance for evaluation of constipation in adults. Do not wait until day 5 or 7 to call, the earlier intervention occurs, the more options are available.
Your telehealth provider at WeightLossInjections.com can evaluate most constipation-related concerns without requiring an in-person visit. A licensed provider can review your current dose, symptom timeline, and OTC history and recommend whether to adjust your titration schedule, add a prescription agent, or investigate further. Access clinical support at [$X/month] for [service detail].
What the Clinical Trial Data Reveal About Constipation Over Time
The SURMOUNT-1 NEJM 2022 trial (Jastreboff et al.) enrolled 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27 with at least one comorbidity, excluding type 2 diabetes) and followed them for 72 weeks. It established the weight-loss efficacy of tirzepatide, 20.9% mean weight reduction at 15 mg versus 3.1% on placebo at 72 weeks, and documented that GI adverse events were predominantly early, predominantly mild to moderate, and predominantly did not lead to treatment discontinuation.
The SURMOUNT-4 JAMA 2023 withdrawal trial is particularly relevant to the constipation timeline question. In SURMOUNT-4, 783 participants completed a 36-week open-label lead-in at maximum maintenance doses (10 or 15 mg). During this lead-in, the period most relevant to understanding what constipation looks like over the medium term, the overall incidence of GI adverse events was 20.7% for constipation in some reporting, predominantly characterized as mild to moderate in severity, with improvement over time. The JAMA 2023 publication confirmed that patients who continued tirzepatide maintained their weight loss and did not develop new or worsening GI safety signals at 88 weeks.
The SURMOUNT-2 Lancet 2023 trial (10 mg and 15 mg in adults with T2D) showed similar GI tolerability patterns, with constipation reported across both dose groups and broadly consistent with the SURMOUNT-1 results, confirming that the adverse event profile is reproducible across trial populations.
The FDA pharmacology review for NDA 217806 provides the mechanistic basis: tirzepatide’s effect on gastric emptying is dose-related, its effect is greatest at treatment initiation and each dose increase, and partial desensitization of the GI response occurs over weeks of sustained exposure. This is the pharmacological explanation for why constipation, while common in the 5 mg window, tends to improve over time and at higher doses.
Zepbound Constipation vs. Other GLP-1 Medications
Constipation is a class-wide GI side effect of incretin-based therapies, but the rates and patterns differ meaningfully between agents.
Among GLP-1 receptor agonists, semaglutide (the active ingredient in Ozempic and Wegovy) also causes constipation, though the FDA-label rates differ by indication and dose. Wegovy (semaglutide 2.4 mg for weight management) reports constipation in approximately 24% of patients per its prescribing information, substantially higher than Zepbound’s 11–17% range — reflecting both the higher dose and the purely GLP-1 mechanism, without the GIP co-activation that characterizes tirzepatide.
Zepbound’s GIP/GLP-1 dual agonism is mechanistically distinct from pure GLP-1 agents. The FDA pharmacology review for NDA 217806 documents that GIP receptor activation has different effects on GI motility than GLP-1 receptor activation — a distinction that may partially account for the inverse constipation-dose relationship seen with tirzepatide (more GIP receptor engagement at higher doses) compared with the dose-proportional GI effects seen with pure GLP-1 agonists. This remains an area of ongoing pharmacological investigation.
The practical takeaway: if you have previously experienced severe constipation on a GLP-1 medication and are transitioning to Zepbound, the constipation profile is different, and at the maximum 15 mg dose, the constipation rate (11%) is notably lower than what Wegovy users experience at 2.4 mg. Conversely, if constipation was not a problem for you on semaglutide, you may still encounter it during the 5 mg phase of Zepbound, the inverse dose-response is a Zepbound-specific pattern, not a GLP-1 class feature.
WeightLossInjections.com: Constipation Management Through Every Step
Our take at WeightLossInjections.com: Constipation is the GI side effect that Zepbound patients most often discover too late — because it doesn’t announce itself as dramatically as nausea or vomiting, it tends to compound quietly over days until it becomes significantly disruptive. The clinical reality is straightforward: if you know it’s coming and have a plan before it starts, it is almost always manageable. The two most important things to do before you get to 5 mg are to establish a daily hydration target (we recommend 2.5 liters as a baseline) and to actively build soluble fiber into your meals, not as a reaction to constipation but as a preemptive habit. The patients who sail through the 5 mg window without significant bowel disruption are the ones who anticipated the drop in food and fluid intake and deliberately compensated for it with fiber and water. The patients who struggle are almost always the ones who didn’t — not because they made a mistake, but because no one told them this was coming. We tell every patient before they start.
At WeightLossInjections.com, [service detail]. Clinical monitoring through every dose escalation step is part of what we provide, including a provider available for telehealth consultation when GI side effects interfere with tolerability or when dose escalation decisions need clinical review. Bundled telehealth + Zepbound access starts at [$X/month].
Frequently Asked Questions
Is constipation worse at higher Zepbound doses?
No, and this is one of the most counterintuitive facts about Zepbound’s GI profile. The Zepbound FDA prescribing information, Table 1 shows that constipation is actually highest at the lowest maintenance dose: 17% at 5 mg, declining to 14% at 10 mg and 11% at 15 mg. Constipation is the only common GI adverse event that decreases as the dose increases, nausea and diarrhea both go up with dose. This means the peak constipation window is the 5 mg phase (typically weeks 5–12), and escalating to higher doses is unlikely to worsen it. If constipation is your main complaint on Zepbound, advancing through the titration schedule as tolerated is clinically reasonable and may actually help.
How long does Zepbound constipation last?
For most patients, pharmacological constipation (driven by slowed colonic transit) resolves within 4–12 weeks at any given dose level as the gut adapts, consistent with the GI tolerability patterns documented in SURMOUNT-1 (Jastreboff et al., NEJM 2022). Nutritional constipation (driven by reduced fiber and fluid intake) does not have a spontaneous resolution timeline, it persists until dietary habits are corrected. If constipation is still significant after 3 months at a stable dose, it is almost certainly nutritional rather than pharmacological, and the intervention is dietary rather than medical.
What laxative is safe to take with Zepbound?
Polyethylene glycol (Miralax) is the preferred first-line OTC laxative for Zepbound-associated constipation. It works osmotically by drawing water into the colon, is non-habit-forming, safe for extended daily use, and has no known pharmacokinetic interactions with tirzepatide. Stool softeners (docusate sodium / Colace) can be added as a second step if stool is hard but transit is adequate. Stimulant laxatives (senna, bisacodyl) are appropriate for rescue use when there has been no bowel movement for 3 or more days, but should not be used daily as routine maintenance. Always use bulk-forming agents like psyllium only with generous concurrent fluid intake, insufficient hydration with psyllium can worsen the problem.
Should I stop Zepbound if I’m constipated?
No — constipation alone is not a clinical reason to stop or reduce Zepbound without provider guidance. Per the Zepbound prescribing information, GI adverse reactions that are mild to moderate in severity and manageable with dietary and OTC interventions do not require treatment discontinuation. Stopping tirzepatide abruptly will not cause withdrawal effects, but it will interrupt your weight loss trajectory and, as SURMOUNT-4 (JAMA 2023) demonstrated, patients who discontinue tirzepatide regain the majority of their lost weight over the following months. Always discuss discontinuation or dose reduction with your prescriber before acting.
Can Zepbound cause both constipation and diarrhea?
Yes — both are listed in the Zepbound FDA prescribing information, Table 1 as adverse reactions, and they can occur in the same patient at different phases of treatment. Constipation is most prominent during the 5 mg window; diarrhea rates are higher at 10 mg and 15 mg. Some patients experience alternating constipation and loose stools as the gut adapts to each new dose level. One important clinical nuance: apparent diarrhea in a patient who has been constipated may represent overflow or paradoxical diarrhea, liquid stool passing around an impaction. If loose stools are accompanied by abdominal bloating and the sense that you haven’t fully evacuated, contact your provider before treating with antidiarrheal medications, as loperamide would worsen an underlying impaction.
Does constipation mean Zepbound is working?
Constipation is not a marker of efficacy, it is a side effect of the drug’s GI mechanism, not of its weight-loss mechanism. Zepbound causes weight loss by suppressing appetite and reducing caloric intake through GIP and GLP-1 receptor activation, per the Zepbound prescribing information and as established in SURMOUNT-1 (Jastreboff et al., NEJM 2022). Patients who experience constipation are not losing weight faster or “responding better” than patients who don’t. Both the patients who get constipated and the patients who don’t can achieve equivalent weight loss results. Managing constipation well actually supports better outcomes by allowing you to maintain adequate nutrition and continue treatment without interruption.
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. Always consult your licensed healthcare provider before making any changes to your medication regimen.