
How Tirzepatide Changes Alcohol Absorption
Alcohol is not directly contraindicated on Zepbound (tirzepatide): the FDA prescribing information lists no direct drug–alcohol pharmacological interaction. However, Zepbound’s signature gastric-emptying delay changes how the body handles alcohol, making the same drink hit harder and later than it did before treatment. Combined GI side effects, compounding dehydration risk, overlapping pancreatitis warnings, and alcohol’s caloric density each independently argue for limiting or avoiding alcohol, especially during the first eight weeks of titration.
Emerging observational data suggest GLP-1 receptor agonists may actually reduce alcohol cravings for some patients; that evidence is preliminary, with no randomized controlled trial in tirzepatide-treated patients as of April 2026.
Medical disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a licensed clinician before changing your alcohol habits while on any prescription medication.
What the FDA Label Says About Alcohol and Zepbound
The Zepbound prescribing information does not list alcohol as a contraindication. Section 7 (Drug Interactions) identifies no direct pharmacological interaction between tirzepatide and alcohol. That absence of a formal contraindication is clinically meaningful, but it is not a green light.
Where the label does speak clearly is in its Warnings and Precautions (Section 5). Two of those warnings overlap substantially with the known risks of alcohol:
- Pancreatitis (Section 5.2): Zepbound carries a warning to discontinue if pancreatitis is suspected; it has not been studied in patients with a history of pancreatitis. Alcohol is independently the second most common cause of acute pancreatitis after gallstones, and heavy alcohol use contributes to 40–70% of chronic pancreatitis cases.
- Acute kidney injury (Section 5.4): GI-mediated fluid loss from nausea, vomiting, and diarrhea can cause dehydration severe enough to produce AKI. Alcohol is a diuretic that independently worsens dehydration, making this a directly additive risk.
WeightLossInjections.com editorial note: “No interaction listed” is not the same as “safe to drink freely.” Zepbound’s mechanism of action, slowing gastric emptying, activating reward-related neural circuits, and causing substantial GI side effects in more than half of patients, changes the risk landscape around alcohol in several important ways that the label’s silence on the topic cannot fully capture. The sections below explain each mechanism.
How Tirzepatide Changes the Way Your Body Handles Alcohol
Gastric Emptying Delay and Alcohol Absorption
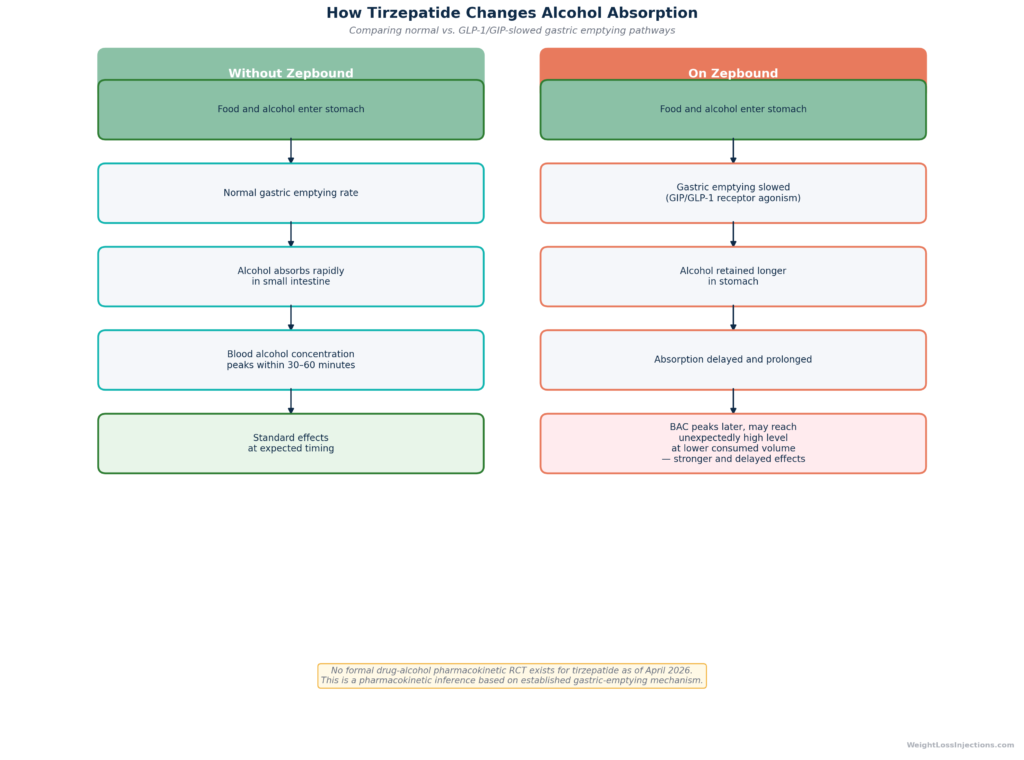
Zepbound’s core mechanism includes slowing gastric emptying, the rate at which the stomach releases its contents into the small intestine, where most alcohol absorption occurs. The Zepbound prescribing information also flags this delay explicitly in the context of oral contraceptives, warning that gastric-emptying delay reduces absorption of other orally consumed compounds and requiring backup contraception during titration.
The same principle applies to alcohol. When gastric emptying is slowed, alcohol consumed with or after food is retained in the stomach longer before reaching the small intestine. The practical effect has two components:
- Delayed onset: The effects of alcohol may be felt later than the patient expects, which can lead to continued drinking before the full effect of the first drink registers.
- Altered peak blood alcohol: Some patients report that a volume of alcohol they previously tolerated produces unexpectedly strong effects once on Zepbound.
It is important to frame this correctly. This is a pharmacokinetic inference based on Zepbound’s established gastric-emptying mechanism, not a finding from a randomized trial. As of April 2026, no published RCT has evaluated tirzepatide’s specific effect on alcohol pharmacokinetics in human patients. The practical implication, that some patients will feel drunk faster or more intensely on the same volume they consumed before starting treatment, is plausible and widely reported in patient communities, but the magnitude of the effect has not been quantified in controlled data.
Nausea and the GI Overlap Problem
GI side effects are the most common adverse events in Zepbound’s clinical program. According to pooled data from SURMOUNT Studies 1 and 2 in the Zepbound prescribing information:
| Adverse Reaction | Placebo | Zepbound 5 mg | Zepbound 10 mg | Zepbound 15 mg |
|---|---|---|---|---|
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation | 5% | 17% | 14% | 11% |
Overall, GI adverse reactions occurred in 56% of pooled Zepbound patients versus 30% of placebo patients, with severe GI adverse events in 3.1% of patients at 15 mg (SURMOUNT-1, NEJM 2022, Jastreboff et al.).
Alcohol is independently a GI irritant. It increases gastric acid secretion, weakens the lower esophageal sphincter (worsening reflux), and can cause nausea, diarrhea, and gastric discomfort in healthy individuals. In a patient already experiencing Zepbound-related nausea, which is most prevalent during weeks 1 through 8 of titration, when the drug is being escalated from 2.5 mg toward therapeutic doses, alcohol adds a second GI stressor on top of an already sensitized system. The combination is particularly problematic because vomiting in this context accelerates dehydration, and dehydration on Zepbound carries the AKI risk flagged in Section 5.4 of the prescribing information.
The Chemoreceptor Trigger Zone Overlap
An additional mechanism connects Zepbound and alcohol-induced nausea. GLP-1 receptor agonists activate the chemoreceptor trigger zone (CTZ) in the area postrema of the brainstem, a brain region without a blood–brain barrier that monitors circulating signals for toxic substances and triggers vomiting. This CTZ activation is the neurological basis of the nausea many Zepbound patients experience, particularly at higher doses. Alcohol can independently activate similar emetic pathways. When both stimuli are present simultaneously, the emetic signal at the CTZ is additive, making nausea and vomiting substantially more likely than with either exposure alone.
Specific Risks: Who Should Be Most Cautious
The population prescribed Zepbound is clinically heterogeneous, a healthy adult taking it for weight loss carries a different risk profile when drinking than a patient with T2D on insulin, or someone taking Zepbound for the OSA indication. The following subsections address each profile individually.
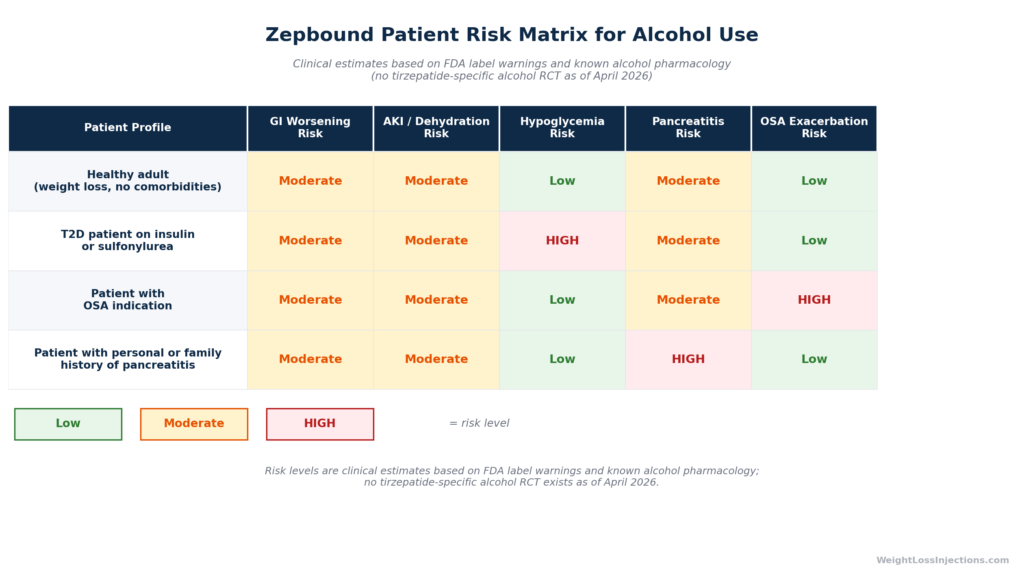
Zepbound Patient Risk Matrix for Alcohol Use
Pancreatitis Risk
The Zepbound label’s pancreatitis warning (Section 5.2) states that patients should discontinue Zepbound if pancreatitis is suspected, and that the drug has not been studied in patients with a history of pancreatitis. This is a box-warning-adjacent precaution that the prescribing clinician must weigh carefully.
Alcohol’s relationship with pancreatitis is well established. It is the second most common trigger of acute pancreatitis after gallstones, and chronic heavy alcohol use is strongly implicated in recurrent and chronic pancreatitis. The biological mechanisms, sphincter of Oddi dysfunction, direct acinar cell toxicity, oxidative stress, and obstruction of pancreatic enzyme secretion, are independent of any drug effect.
When both Zepbound’s mechanism and alcohol’s mechanism are present simultaneously, the risk of pancreatic stress is at minimum additive. As of April 2026, no randomized data specifically quantifies this combined risk in tirzepatide patients. That absence of data is not reassuring, it simply means the signal has not been studied, not that the risk does not exist. Patients with any personal or family history of pancreatitis, gallstones, or hypertriglyceridemia should discuss alcohol avoidance explicitly with their prescribing provider before their first drink on Zepbound.
Acute Kidney Injury Risk
The Zepbound prescribing information Section 5.4 warns that GI-mediated fluid loss can cause dehydration leading to acute kidney injury, and calls for appropriate hydration and monitoring of renal function when GI side effects are severe. Alcohol suppresses antidiuretic hormone (ADH) secretion, producing diuresis, the excretion of additional fluid, even when baseline hydration is adequate. A Zepbound patient experiencing vomiting or diarrhea who is simultaneously drinking alcohol is at compounded risk for the kind of dehydration that precedes AKI. Early warning signs, significantly decreased urine output, concentrated dark urine, back or flank pain, or lower-extremity swelling, warrant same-day provider contact.
Hypoglycemia in Patients on Insulin or Sulfonylureas
Zepbound itself has a low independent risk of hypoglycemia in most patients. However, the Zepbound prescribing information Section 5.3 identifies substantially elevated hypoglycemia risk in patients who are concurrently taking insulin or sulfonylureas, and recommends dose reduction of those agents when initiating Zepbound.
Alcohol adds a separate hypoglycemia mechanism: it suppresses hepatic gluconeogenesis, the liver’s process of producing glucose to maintain blood sugar during fasting. Normally, the liver compensates for declining blood glucose by generating new glucose, alcohol blunts this response. In a patient on insulin or a sulfonylurea who has been drinking and has not eaten recently, this alcohol-induced suppression of gluconeogenesis, combined with the insulin secretagogue or direct insulin effect, creates a significant hypoglycemia risk that can persist for several hours after the last drink and be masked by the sedative effects of alcohol. These patients should be particularly cautious and may benefit from reviewing their monitoring protocol with their provider before any alcohol use.
Sleep Apnea Patients
Zepbound’s OSA indication, approved by the FDA on December 20, 2024, making it the first and only prescription medicine for moderate-to-severe OSA in adults with obesity, introduces a particularly important alcohol consideration. In the SURMOUNT-OSA trials (NEJM 2024), tirzepatide reduced the apnea-hypopnea index (AHI) by an average of 25.3 events per hour in Trial 1 (patients not on PAP therapy), with 42% of tirzepatide patients achieving OSA remission versus 16% on placebo.
Alcohol independently worsens sleep apnea through at least three mechanisms: relaxation of upper airway muscles (including the genioglossus and pharyngeal dilators), reduced arousal response to hypoxia, and increased nasal and pharyngeal congestion. Drinking before sleep in a patient with existing OSA can substantially increase AHI and lower nocturnal oxygen saturation, undoing hours of Zepbound-mediated improvement. Patients prescribed Zepbound for the OSA indication should strongly consider avoiding alcohol in the hours before sleep and discuss a specific guidance protocol with their prescribing provider.
Practical Guidance: How to Minimize Risk if You Choose to Drink
No published Zepbound-specific clinical guideline establishes a safe dose of alcohol for patients on tirzepatide. The following recommendations apply current CDC/USDA Dietary Guidelines as a reference point while accounting for Zepbound’s specific risk profile. The appropriate individual level requires a conversation with your prescribing provider.
- Avoid alcohol entirely during the first 4–8 weeks of treatment. This is the peak period for GI side effects, the window when the gastric-emptying effect is most physiologically prominent, and the time when the drug interaction with food absorption is being established. The Zepbound titration schedule takes a minimum of 20 weeks to reach 15 mg, with a new dose increase every 4 weeks; GI side effects tend to spike with each escalation.
- If you do drink, do not do so on an empty stomach. Empty-stomach alcohol is absorbed more rapidly regardless of Zepbound status; combined with gastric-emptying delay, the pharmacokinetics become unpredictable. Eat a substantial meal before any alcohol.
- Use dietary guideline amounts as a ceiling, not a target. The CDC guideline for moderate drinking — up to 1 standard drink per day for women, up to 2 per day for men — represents an upper limit for healthy adults. Patients on Zepbound have pharmacokinetic reasons to consume less than they otherwise would.
- Avoid high-sugar cocktails. Added sugars in mixed drinks independently worsen nausea and osmotic diarrhea in patients on GLP-1 receptor agonists, and they undercut the caloric-deficit goal of treatment.
- Hydrate aggressively on any day you drink. Counter alcohol’s diuretic effect and Zepbound’s dehydration risk simultaneously by drinking at least one glass of water for every standard drink consumed, in addition to baseline daily hydration.
- If alcohol hits you dramatically harder than before starting Zepbound, stop. The gastric-emptying delay means the full effect may not be apparent for longer than usual — stop drinking and do not try to “catch up” to a previous tolerance level. Discuss the change with your provider.
- Never drink when you have active GI symptoms. If you are experiencing nausea, vomiting, or diarrhea from your current dose, adding alcohol will worsen symptoms, increase dehydration risk, and may require medical attention.
Does Zepbound Reduce Alcohol Cravings?
One of the more intriguing, and widely reported, observations from patients using GLP-1 receptor agonists is that many find their desire to drink alcohol significantly reduced. This is not a coincidence or a placebo effect, and its proposed biological mechanism is substantive, even if the clinical evidence remains early-stage.
The Dopamine Reward Pathway Hypothesis
GLP-1 receptors are expressed in the mesolimbic dopamine system, specifically in the ventral tegmental area (VTA) and nucleus accumbens, the brain’s core reward circuit. GLP-1 receptor agonists, including tirzepatide, modulate dopaminergic signaling in this pathway, reducing the reinforcing properties of highly palatable food. The same circuit mediates the rewarding properties of alcohol, drugs of abuse, and other addictive stimuli. Pharmacologically reducing the reward value of one substance through GLP-1 receptor activation may, in parallel, reduce the subjective craving for others — including alcohol.
Animal studies have shown that GLP-1 receptor agonists reduce alcohol consumption and preference in rodent models. The translational evidence in humans is newer but emerging.
What the Human Evidence Actually Shows
A 2023 analysis examining over 68,200 social media posts from Reddit and Twitter (X) found self-reported reductions in alcohol intake and alcohol-related cravings among GLP-1 receptor agonist users, including both semaglutide and tirzepatide, with a substantial proportion of users describing the change as unexpected and unsolicited, not something they were trying to achieve (Hankir & Bhatt, analysis of social media self-reports, 2023). Social media self-report data is not clinical evidence, but the volume and consistency of unprompted reports across user communities is notable.
Several published case series and observational reports in peer-reviewed literature describe individual patients who substantially reduced or eliminated alcohol use while on GLP-1 receptor agonists without making any deliberate effort to do so. A 2024 retrospective cohort study examining electronic health records found reduced alcohol-related diagnoses and hospitalizations in patients who initiated GLP-1 receptor agonist therapy compared with matched controls, though confounding by prescriber behavior and patient selection cannot be excluded.
What the Evidence Does Not Yet Support
As of April 2026, no randomized controlled trial has specifically evaluated tirzepatide for alcohol use disorder (AUD) or alcohol craving reduction. Zepbound is not approved or recommended as a treatment for AUD. The FDA has not reviewed a New Drug Application for tirzepatide in this indication. Using Zepbound to manage alcohol dependence, without appropriate clinical oversight, behavioral support, and potentially concurrent AUD-specific pharmacotherapy, would be clinically inappropriate.
The appropriate framing: if you are taking Zepbound for weight management or OSA and notice that your desire to drink alcohol has diminished, that is a potentially beneficial pharmacological side effect consistent with the known biology. It is not a reason to seek out Zepbound as a primary AUD treatment, and it does not change the risk-management guidance above for patients who continue to drink.
Decision Flowchart: Is It Safe for Me to Drink on Zepbound?
Alcohol, Calories, and Weight Loss Progress
Beyond the safety considerations, alcohol creates a third category of concern specific to patients using Zepbound for weight management: it undermines the very outcomes the medication is designed to produce.
The calorie math is unfavorable. Each gram of alcohol contains approximately 7 kilocalories, higher than carbohydrates or protein (4 kcal/g each) and approaching fat (9 kcal/g). Unlike fat, protein, or carbohydrates, alcohol calories carry no nutritional value. A single 5-ounce glass of wine contains approximately 120–125 kcal; a 12-ounce regular beer approximately 145–155 kcal; a standard cocktail with a sugary mixer frequently exceeds 200 kcal. Regular drinking can meaningfully offset the caloric deficit that Zepbound’s appetite suppression is working to establish.
The appetite mechanism is disrupted. One of Zepbound’s key benefits is a reduction in appetite and food-reward signaling. Alcohol, by contrast, increases appetite through several mechanisms, reducing leptin levels, stimulating orexigenic peptides, and lowering dietary inhibition at the prefrontal cortex level. A patient who drinks significantly may find that Zepbound’s appetite suppression is partially overridden, especially if drinking leads to post-drinking overeating (“the munchies” phenomenon).
SURMOUNT-1 trial weight-loss context. Patients on 15 mg tirzepatide achieved an average 20.9% reduction in body weight at 72 weeks versus −3.1% on placebo in SURMOUNT-1 (NEJM 2022), with 57% of patients losing 20% or more. These outcomes were achieved in the context of reduced-calorie diet and increased physical activity per the trial protocol. Regular alcohol use was not studied as a variable, but its caloric load and appetite-stimulating effects are pharmacologically inconsistent with maximizing those outcomes.
The bottom line: even amounts of alcohol that fall within current CDC dietary guidelines can slow or plateau weight loss progress in a patient on Zepbound. This is not a safety risk per se, but it is worth factoring into the personal decision about whether, and how often, to drink.
Zepbound GI Adverse Event Rates by Dose vs. Alcohol’s Independent GI Effects
What to Watch For: Symptoms That Require Provider Contact
If you choose to drink while on Zepbound, the following signs after alcohol consumption warrant same-day provider contact or, where urgent, emergency evaluation:
Contact your WeightLossInjections.com telehealth provider:
- Severe or prolonged nausea and vomiting beyond what you typically experience on Zepbound
- Significantly decreased urine output or very dark urine (signs of dehydration and possible AKI)
- Upper abdominal pain — especially if it radiates to the back (possible pancreatitis signal)
- Symptoms of hypoglycemia: shakiness, sweating, confusion, unusual hunger, heart palpitations (in patients on insulin or sulfonylureas)
- Alcohol effects that were dramatically stronger than expected, even from small quantities
Seek emergency care immediately:
- Severe upper abdominal pain with nausea and vomiting that does not resolve (acute pancreatitis emergency)
- Signs of severe dehydration: dizziness on standing, inability to urinate for many hours, extreme weakness
- Any symptoms of severe hypoglycemia that do not resolve with oral glucose
Our Take at WeightLossInjections.com
Alcohol is the most common question patients ask about lifestyle restrictions on Zepbound, and understandably so, because the answer is genuinely more nuanced than a simple yes or no. The FDA prescribing information’s silence on alcohol does not mean there is no risk. It means the risk is indirect, distributed across multiple mechanisms, and dependent on patient-specific factors: dose level, titration phase, comorbidities, concurrent medications, and volume consumed.
Our clinical approach at WeightLossInjections.com is pragmatic. We do not categorically prohibit alcohol for every Zepbound patient, some patients, at stable maintenance doses, without the specific comorbidities outlined above, and drinking at moderate levels while hydrated and after a meal, are making a defensible choice. We do counsel every patient to avoid alcohol entirely during titration; to understand that their previous alcohol tolerance is no longer a reliable guide; and to recognize the pancreatitis, AKI, and OSA risks as real signal, not theoretical worry.
For patients starting Zepbound through our platform — [$X/month] for bundled telehealth and medication coordination, [service detail] — the pre-treatment intake includes a review of alcohol use history as a standard clinical consideration. If alcohol use disorder or heavy drinking is part of the picture, that changes the clinical approach substantially and warrants specialized support alongside Zepbound, not instead of it. Our licensed providers will give you a personalized assessment based on your complete health history, not generic web guidance.
Take our free eligibility quiz at WeightLossInjections.com to get started.
Frequently Asked Questions
Can you drink alcohol while on Zepbound?
Alcohol is not directly contraindicated on Zepbound, the FDA prescribing information lists no direct pharmacological interaction. However, alcohol can worsen Zepbound’s GI side effects, increase pancreatitis and kidney injury risk, compound dehydration, impair weight loss progress, and, in patients prescribed for OSA, worsen sleep apnea events. Most providers recommend limiting or avoiding alcohol, particularly during the first 4–8 weeks of titration. Individual guidance depends on your health history and concurrent medications.
Does alcohol affect how Zepbound works?
Alcohol does not block tirzepatide’s mechanism of action or reduce its efficacy directly. However, alcohol’s empty calories, appetite-stimulating effects, and behavioral impact on dietary inhibition can counteract the appetite suppression and caloric deficit that Zepbound is designed to facilitate. Over time, regular alcohol use may meaningfully slow or plateau weight loss progress, even without a pharmacological interaction.
Why do I feel drunk faster on Zepbound?
Zepbound slows gastric emptying, the rate at which food and liquids leave the stomach and enter the small intestine where alcohol is primarily absorbed. When this process is slower, alcohol takes longer to reach peak blood concentration but may reach a higher level from the same volume than it would in a person with normal gastric motility. This is a pharmacokinetic effect, not a formal drug interaction; no published clinical trial has quantified the magnitude of this effect specifically for tirzepatide as of April 2026. If you find the same amount of alcohol produces dramatically stronger effects than before starting Zepbound, that is a real phenomenon consistent with this mechanism — reduce your intake accordingly and discuss it with your provider.
Can Zepbound and alcohol cause pancreatitis?
Both Zepbound and alcohol independently carry a risk of pancreatitis. The Zepbound prescribing information Section 5.2 warns to discontinue the drug if pancreatitis is suspected, and states it has not been studied in patients with a pancreatitis history. Alcohol is the second most common cause of acute pancreatitis and a leading cause of chronic pancreatitis. Combining the two may increase risk in an additive manner, though no randomized trial has studied this specific combination in tirzepatide patients as of April 2026. Patients with any personal or family history of pancreatitis should avoid alcohol entirely on Zepbound.
Does Zepbound reduce alcohol cravings?
Emerging observational evidence, including analysis of self-reports across large social media datasets and several retrospective cohort studies, suggests that GLP-1 receptor agonists including tirzepatide may reduce alcohol cravings and intake via modulation of dopamine signaling in the mesolimbic reward pathway. This is consistent with the known biology of GLP-1 receptors in the brain’s reward circuit. However, as of April 2026, no randomized controlled trial has specifically evaluated tirzepatide for alcohol use disorder. Zepbound is not FDA-approved and should not be used as a treatment for alcohol use disorder. Patients who notice reduced alcohol cravings while on Zepbound should report this to their provider as a relevant observation; it does not change the safety guidance above.
How long should I wait to drink after my Zepbound injection?
No specific waiting period is established in the Zepbound prescribing information. GI side effects, including nausea and vomiting, are highest in the 24–48 hours following an injection and during dose escalation periods. Tirzepatide’s half-life is approximately 5–6 days, meaning the drug is pharmacologically active throughout the entire week between doses, not just in the days immediately post-injection. If you choose to drink, doing so several days after your weekly injection, when GI side effects are typically at their weekly low, reduces the risk of compounded nausea. Discuss timing with your prescribing provider, especially during titration.