
Zepbound Full Titration Chart
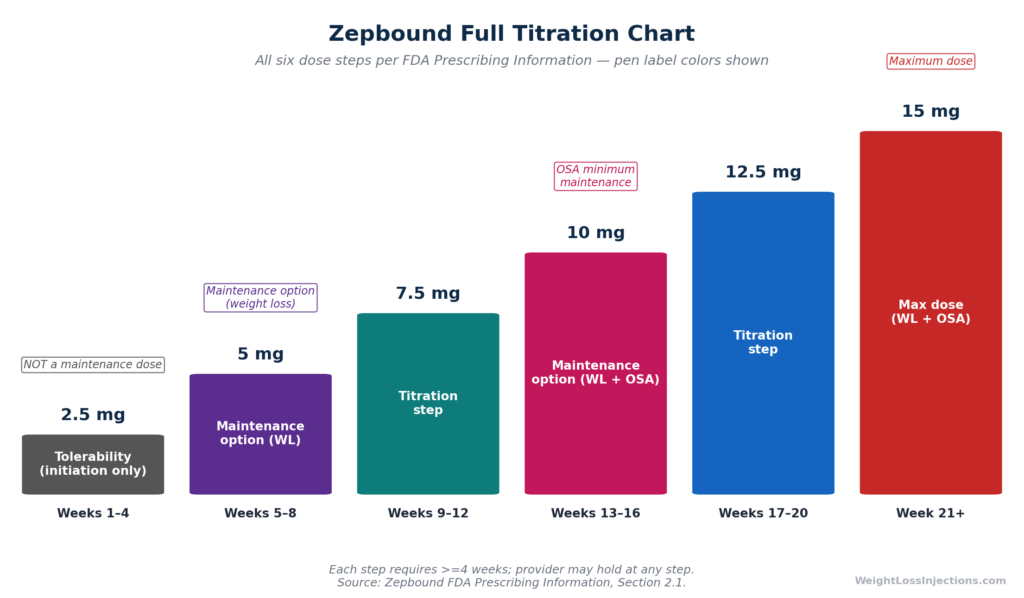
Zepbound (tirzepatide) starts at 2.5 mg once weekly for 4 weeks, a tolerability step only, then increases in 2.5 mg increments every ≥4 weeks up to a maximum of 15 mg/week. Approved maintenance doses for weight loss are 5 mg, 10 mg, or 15 mg; the obstructive sleep apnea (OSA) indication requires 10 mg or 15 mg. Clinical trial data from SURMOUNT-1 show meaningful weight loss at every maintenance dose level, ranging from −15.0% at 5 mg to −20.9% at 15 mg at 72 weeks.
The Complete Zepbound Dosage Chart (Weight Loss)
Tirzepatide is the only approved anti-obesity medication that requires progression through six distinct dose strengths before reaching a maximum. That design is intentional: each 2.5 mg step allows the GI tract to adapt before further escalation. Getting the schedule right improves tolerability and long-term adherence.
The table below is the complete weight-loss titration sequence per Zepbound FDA Prescribing Information, Section 2.1:
| Week Range | Dose | Clinical Purpose | Approved Maintenance Dose? |
|---|---|---|---|
| Weeks 1–4 | 2.5 mg | Tolerability initiation only | No |
| Weeks 5–8 | 5 mg | First therapeutic level | Yes (weight loss) |
| Weeks 9–12* | 7.5 mg | Titration step | No |
| Weeks 13–16* | 10 mg | Second maintenance option | Yes (weight loss + OSA) |
| Weeks 17–20* | 12.5 mg | Titration step | No |
| Week 21+* | 15 mg | Maximum dose; third maintenance option | Yes (weight loss + OSA) |
*Each asterisked step requires a minimum of 4 weeks at the preceding dose before increasing. Providers may hold at any step based on individual tolerability. Total time to reach 15 mg: minimum 20 weeks. Source: Zepbound prescribing information.
Key Points About the 2.5 mg Starting Dose
The 2.5 mg dose is explicitly not an approved maintenance dose for weight reduction or OSA. Its sole purpose is to minimize GI side effects, primarily nausea, vomiting, and diarrhea, by allowing gradual receptor adaptation. Clinically meaningful weight loss does not typically occur at 2.5 mg. Patients sometimes interpret the absence of early weight loss as treatment failure; it is not. Per Zepbound prescribing information, Section 2.1, meaningful weight reduction begins at the 5 mg maintenance level.
Maintenance Doses: 5 mg, 10 mg, and 15 mg
Three doses are FDA-approved as maintenance levels for chronic weight management: 5 mg, 10 mg, and 15 mg. The 7.5 mg and 12.5 mg doses exist only as titration steps, they are not approved maintenance doses. This matters clinically: a patient experiencing excellent tolerability at 7.5 mg should still progress to 10 mg (the next maintenance dose) per FDA press release approving Zepbound unless a specific clinical reason justifies staying lower.
Zepbound Dosage Chart for Obstructive Sleep Apnea (OSA)
Zepbound received its second FDA approval on December 20, 2024, becoming the first and only prescription medication approved for moderate-to-severe obstructive sleep apnea in adults with obesity, per Eli Lilly OSA approval press release. The dosing sequence follows the same ladder, but the maintenance requirements differ.
How OSA Titration Differs from Weight Loss
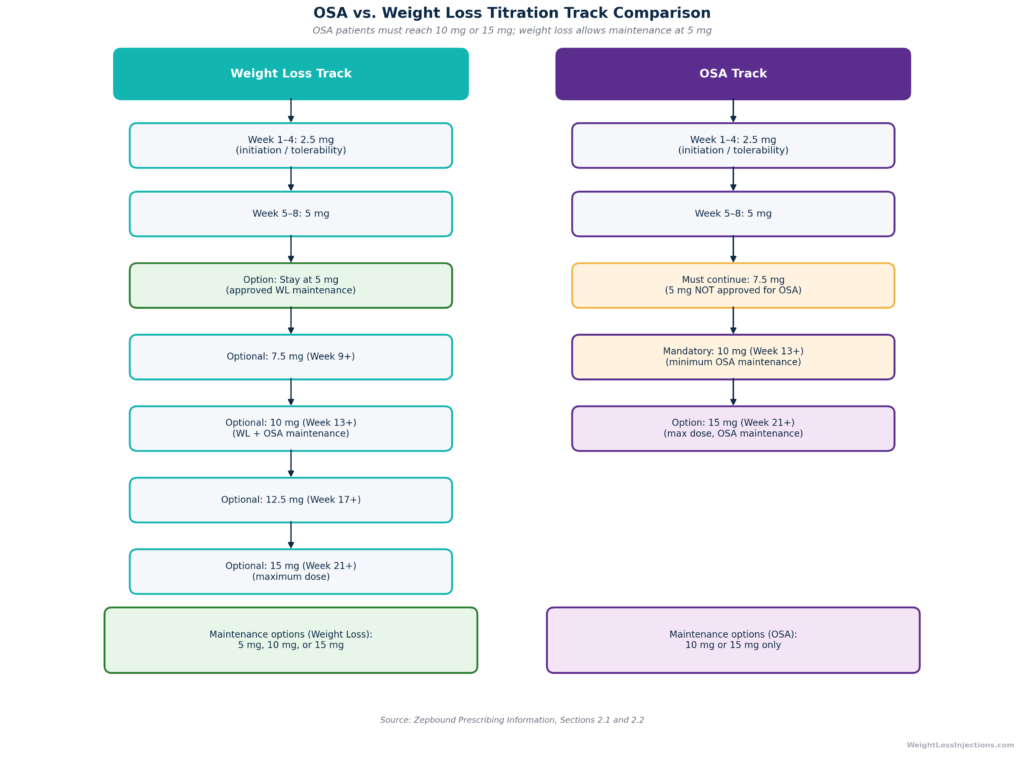
The opening titration sequence is identical for both indications: start at 2.5 mg for 4 weeks, then advance to 5 mg for 4 weeks. After that, the two pathways diverge.
| Parameter | Weight Loss Indication | OSA Indication |
|---|---|---|
| Starting dose | 2.5 mg × 4 weeks | 2.5 mg × 4 weeks |
| After week 8 | May maintain at 5 mg | Must continue titrating |
| Required next step (week 9+) | Provider discretion | 7.5 mg mandatory step |
| Minimum OSA maintenance dose | N/A | 10 mg |
| Approved maintenance doses | 5 mg, 10 mg, or 15 mg | 10 mg or 15 mg only |
| Maximum dose | 15 mg | 15 mg |
Per Zepbound prescribing information, Section 2.2, 5 mg is not an FDA-approved maintenance dose for OSA. Patients using Zepbound for sleep apnea must reach at least 10 mg before stopping titration. Providers prescribing for OSA should note that the flexibility to maintain at 5 mg, permissible for weight loss, does not apply to this indication.
The evidence base for the OSA approval comes from the SURMOUNT-OSA program: two parallel 52-week randomized controlled trials in 469 adults with moderate-to-severe OSA (apnea-hypopnea index ≥15 events/hour) and obesity. In the no-PAP-therapy arm, tirzepatide reduced AHI by 25.3 events/hour versus 5.3 events/hour for placebo, and 42% of tirzepatide patients no longer had moderate-to-severe OSA at 52 weeks, compared to 16% on placebo, per Eli Lilly OSA press release.
Dose-Specific Efficacy: What the Trials Show
Choosing a maintenance dose is not just a tolerability question, each dose produces a meaningfully different weight-loss outcome. The pivotal data come from two published phase 3 trials.
SURMOUNT-1: Non-Diabetic Obesity (72 Weeks)
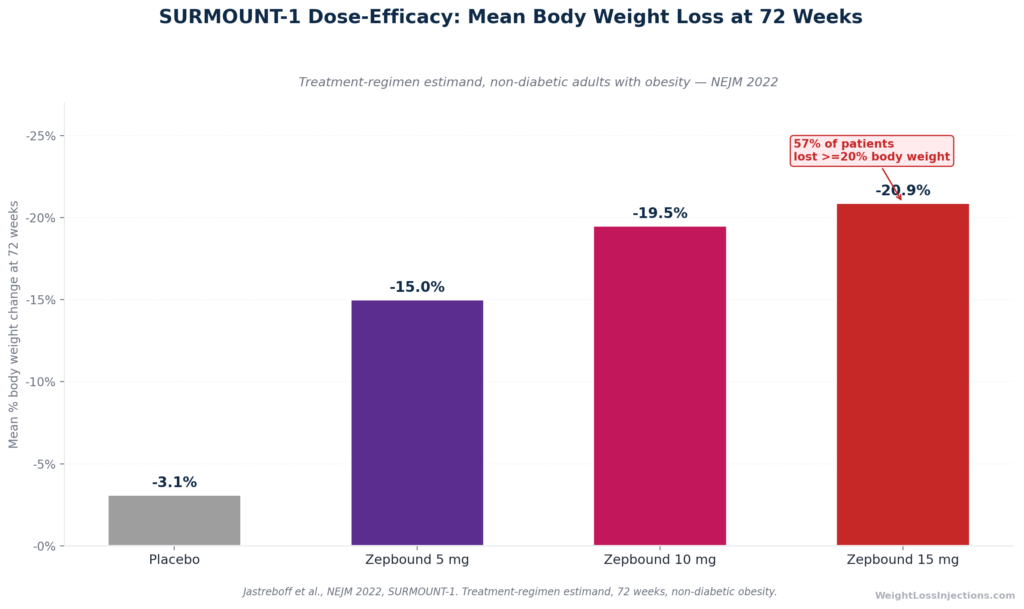
SURMOUNT-1 enrolled 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one comorbidity, excluding type 2 diabetes. Results at 72 weeks (treatment-regimen estimand) per SURMOUNT-1 published in NEJM 2022, Jastreboff et al.:
| Group | Mean Body Weight Change at 72 Weeks | ≥20% Weight Loss |
|---|---|---|
| Placebo | −3.1% | 3% |
| Zepbound 5 mg | −15.0% | — |
| Zepbound 10 mg | −19.5% | — |
| Zepbound 15 mg | −20.9% | 57% |
The incremental difference between doses is real but diminishing: moving from 5 mg to 10 mg adds approximately 4.5 percentage points of mean weight loss; moving from 10 mg to 15 mg adds roughly 1.4 additional percentage points. At 15 mg, 57% of participants lost 20% or more of their body weight and 91% lost at least 5%, per SURMOUNT-1 in NEJM 2022.
The clinical significance of 5 mg should not be understated. A mean loss of 15.0% of body weight at the lowest maintenance dose, nearly five times the placebo response, is clinically meaningful by any obesity pharmacotherapy benchmark. For a 220-pound (100 kg) patient, that represents approximately 33 pounds (15 kg) of mean weight reduction.
SURMOUNT-1 Dose-Efficacy Bar Chart
SURMOUNT-2: Obesity with Type 2 Diabetes (72 Weeks)
In patients with both obesity and type 2 diabetes, weight loss potential is moderately lower, consistent with known biology of insulin resistance and diabetes pharmacotherapy interactions. SURMOUNT-2 enrolled 938 adults (BMI ≥27, HbA1c 7–10%) and tested only the 10 mg and 15 mg doses against placebo. Results per SURMOUNT-2 published in Lancet 2023:
- 10 mg: −12.8% mean body weight (vs. −3.2% placebo)
- 15 mg: −14.7% mean body weight (vs. −3.2% placebo)
Additionally, 49% of tirzepatide-treated patients achieved normoglycemic HbA1c below 5.7% at 72 weeks, per ACC SURMOUNT-2 clinical trial summary. For patients with T2D starting Zepbound for weight management, the same titration schedule applies, the underlying metabolic context changes the magnitude of weight response, not the dosing protocol.
The Takeaway on Dose Selection
Not every patient needs 15 mg. The data confirm that 5 mg produces clinically significant weight loss in patients without T2D, and that 10 mg gets most patients to the threshold of major response. The 15 mg dose maximizes outcomes, particularly the proportion of patients achieving ≥20% weight loss, but comes with incrementally higher rates of GI adverse events. Per Zepbound prescribing information, Table 1, severe GI adverse events occurred in 1.7% of patients at 5 mg, 2.5% at 10 mg, and 3.1% at 15 mg, compared to 1.0% on placebo. The goal should be the lowest dose that achieves the patient’s weight-management objectives with acceptable tolerability.
Pen Color Codes by Dose
Zepbound single-dose auto-injector pens use color-coded labels to differentiate the six dose strengths. This is a critical safety feature: dispensing errors have been reported when patients confuse strengths. The color system per Zepbound pen Instructions for Use:
| Dose | Pen Label Color | Maintenance Dose? |
|---|---|---|
| 2.5 mg | Dark gray | No (tolerability initiation only) |
| 5 mg | Dark purple | Yes (weight loss) |
| 7.5 mg | Dark teal | No (titration step) |
| 10 mg | Pink | Yes (weight loss + OSA) |
| 12.5 mg | Blue | No (titration step) |
| 15 mg | Red | Yes (weight loss + OSA) |
Every pen contains 0.5 mL of solution regardless of strength, concentration varies by dose, not volume. Before each injection, verify that the label color on your pen matches your current prescribed dose. If your pharmacy dispenses a different color than your previous supply, confirm the dose with your provider before injecting.
Device Options: Single-Dose Pen, Vial, and KwikPen
As of April 2026, Zepbound is available in three delivery formats:
- Single-dose auto-injector pen: The original format. One pen equals one weekly dose. Available in all six strengths, color-coded as above. Features a two-click confirmation system, the first click starts delivery, the second click confirms completion. Hold for up to 10 seconds. Per Zepbound pen Instructions for Use.
- Single-dose vial: Each vial contains one dose (0.5 mL) and requires a separate syringe and needle purchased separately. Available in all six strengths through LillyDirect. Initially launched in April 2024 for 2.5 mg and 5 mg; all six strengths became available by mid-2025.
- Multi-dose KwikPen (launched February 23, 2026): A single-patient-use pen containing 4 weekly doses, one month of treatment per pen. FDA label expansion approved February 2026. Currently available only through LillyDirect for self-pay patients; not yet available through traditional pharmacies, per CNBC, February 23, 2026.
Dosage Adjustments: When to Stay at a Lower Dose
The titration schedule is a framework, not a mandate. Both the FDA label and clinical practice support staying at lower doses when circumstances warrant.
Tolerability-Based Dose Hold
If GI side effects, nausea, diarrhea, vomiting, constipation, are present and unresolved after ≥4 weeks at a current dose, a provider may hold at that dose for an additional 4 weeks before attempting to escalate. Per Zepbound prescribing information, Section 2.1, if a maintenance dose is not tolerated, the provider may also reduce to the previous dose. This reduction to a lower maintenance level is explicitly permitted under the FDA label, it is not off-label practice.
Managing GI effects by adjusting titration pace is well-supported clinically. The four-week minimum at each step is a floor, not a target; patients with persistent side effects may benefit from extending to 6–8 weeks at a given dose before stepping up.
Staying at 5 mg or 10 mg Long-Term
If a patient is achieving their weight-management goals at 5 mg or 10 mg with acceptable tolerability, there is no clinical rationale to increase further. SURMOUNT-4 demonstrated that weight is maintained, and continues to decline, when patients remain on tirzepatide long-term, per SURMOUNT-4 published in JAMA 2023. The same trial showed that discontinuing tirzepatide, at any maintenance dose, results in substantial weight regain: patients who switched to placebo after a 36-week lead-in regained an average of 14.0% of body weight over the subsequent 52 weeks. This underscores that Zepbound is a long-term treatment, not a finite course.
Dose Reduction After Tolerability Issue
The label permits reducing from, for example, 10 mg back to 7.5 mg (a titration-step dose), or from 15 mg back to 12.5 mg, if a maintenance dose proves intolerable after an extended attempt. This is not considered a failure of the protocol, it reflects appropriate personalization of chronic disease management.
Missed Dose Rules
Zepbound is a once-weekly injection with a pharmacokinetic half-life of approximately 5–6 days. That long half-life means a single missed dose does not immediately eliminate drug exposure, but the protocol for missed doses is specific and should be followed precisely, per Zepbound prescribing information, Section 2.3:
| Time Since Missed Dose | Action |
|---|---|
| ≤4 days (96 hours) since scheduled day | Administer as soon as possible; resume regular weekly schedule |
| >4 days (>96 hours) since scheduled day | Skip this dose entirely; resume on next regularly scheduled day |
| Any circumstance | Never administer two doses in one week to compensate |
Practical tip: Choose a consistent injection day, same day of the week, same time, and set a recurring reminder. If you travel and need to shift injection day, the label permits changing days as long as the old and new injection days are at least 3 days (72 hours) apart, per Zepbound prescribing information.
Self-Pay Cost by Dose (LillyDirect, Verified April 2026)
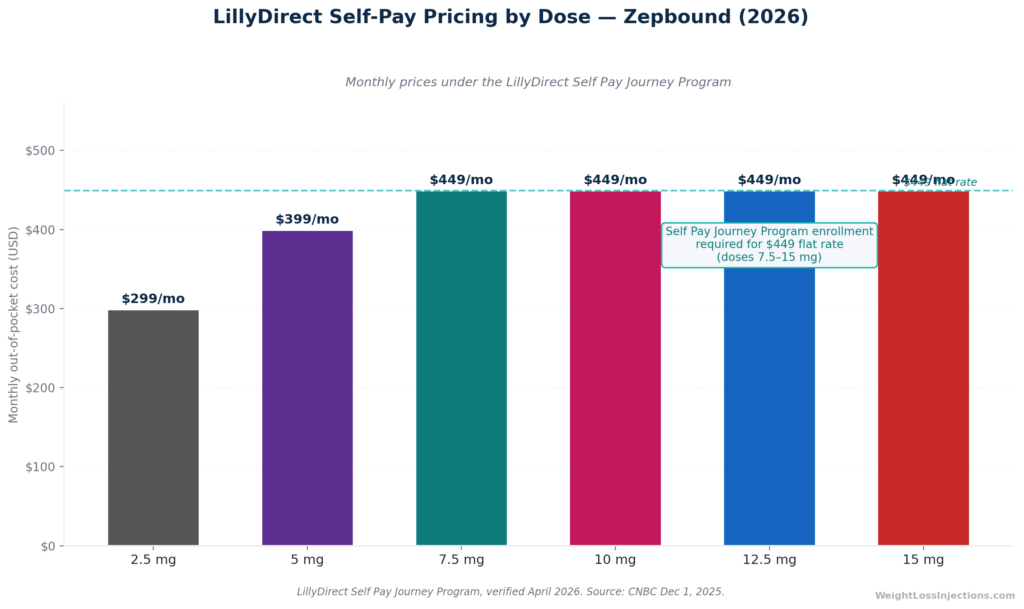
Zepbound’s list price (WAC) is $1,086/mo for a 28-day supply across all dose strengths, applicable to all six doses, from 2.5 mg to 15 mg, at retail pharmacies, per Eli Lilly pricing page. Most patients do not pay this rate.
Through the LillyDirect Self Pay Journey Program (enrollment required), self-pay pricing is structured by dose tier, effective December 1, 2025, per CNBC, December 1, 2025:
| Dose | LillyDirect Self-Pay Price/Month (Journey Program) |
|---|---|
| 2.5 mg | $299/mo |
| 5 mg | $399/mo |
| 7.5 mg | $449/mo |
| 10 mg | $449/mo |
| 12.5 mg | $449/mo |
| 15 mg | $449/mo |
For patients on commercial insurance with Zepbound coverage, the Zepbound savings card can reduce out-of-pocket cost to as low as $25/mo (with commercial plan coverage; subject to annual program maximums and a limit of 13 fills per calendar year for 2026), per Zepbound savings card terms.
Medicare coverage note: Medicare is currently prohibited from covering Zepbound for the weight management indication. However, Medicare Part D plans may cover Zepbound for patients prescribed specifically for moderate-to-severe OSA. A temporary Medicare GLP-1 Bridge program (July–December 2026) provides coverage at a $50 copayment for eligible enrollees with BMI ≥35 or ≥27 with clinical criteria, per KFF analysis, March 2026.
LillyDirect Self-Pay Pricing by Dose
Injection Technique Quick Reference
Correct injection technique does not change as the dose increases, only the pen color changes. The following protocol applies at all dose levels, per Zepbound single-dose pen Instructions for Use.
Approved Injection Sites
Three sites are approved for subcutaneous Zepbound injection: abdomen (stomach), outer thigh, and back of upper arm. Patients self-injecting can use the abdomen or thigh without assistance. Injection into the upper arm requires another person’s help. Rotate injection sites weekly, injecting the same anatomical location repeatedly can cause lipohypertrophy, which impairs drug absorption.
Timing
Once weekly. The same day each week is recommended for consistency. Any time of day is acceptable; injection with or without food is permitted. The drug’s ~5–6-day half-life means minor variations in injection timing (a few hours) do not materially affect plasma levels, per Zepbound prescribing information.
Oral Contraceptive Interaction
For patients using oral contraceptives, Zepbound’s delayed gastric emptying effect can reduce oral drug absorption — including hormonal pills. Per Zepbound prescribing information, use a backup or non-oral contraceptive method for 4 weeks after initiating Zepbound and for 4 weeks after each dose increase.
Storage at Each Dose
Storage requirements do not vary by dose strength. Refrigerate at 2°C–8°C (36°F–46°F) in the original carton. Each pen may be stored at room temperature not exceeding 30°C (86°F) for up to 21 days; once at room temperature, do not return to the refrigerator. Never freeze. Inspect the solution before each injection, it should be colorless to slightly yellow and free of particles, per Zepbound prescribing information.
Compounding Status: A Note for 2026
Patients researching Zepbound dosing sometimes encounter references to compounded tirzepatide, which was available from certain pharmacies during the FDA-declared drug shortage. That window is closed. The tirzepatide shortage was formally resolved on December 19, 2024, per FDA memorandum, December 19, 2024. Enforcement discretion for 503A compounding pharmacies ended February 18, 2025; for 503B outsourcing facilities, March 19, 2025, per FDA clarification page. As of April 2026, compounding essentially identical tirzepatide is not permissible. Only the FDA-approved Zepbound product, in single-dose pen, single-dose vial, or KwikPen format — is legally available for general dispensing.
OSA vs. Weight Loss Titration Track Comparison
Our take at WeightLossInjections.com: The Zepbound titration chart is not one-size-fits-all. The minimum 20-week path to 15 mg is a floor, not a target. Our experience with [service detail] is that patients who are allowed to progress at their own tolerability pace are more likely to stay on therapy long enough to reach and sustain meaningful weight loss. The trial data are clear: 5 mg works, 10 mg works better for most, and 15 mg maximizes outcomes for those who tolerate it. What fails is abandoning the medication during the early titration phase because of GI side effects that could have been managed with a longer hold at a lower dose. WeightLossInjections.com telehealth providers work with you to customize your titration schedule, monitor side effects, and adjust as needed, all included in our program starting at [$X/month].
Frequently Asked Questions
What is the starting dose of Zepbound?
The starting dose is 2.5 mg once weekly for the first 4 weeks. This is a tolerability initiation step only, it is not an approved maintenance dose for weight loss or OSA, and it is not expected to produce significant weight loss on its own. Per Zepbound prescribing information, Section 2.1, 2.5 mg exists solely to allow GI adaptation before advancing to the first therapeutic dose of 5 mg.
How long does it take to reach the maximum dose of 15 mg?
At minimum, 20 weeks — five consecutive 4-week steps. In practice, many patients take longer: if GI side effects require holding at a step for 6–8 weeks before escalating, the timeline extends accordingly. There is no clinical mandate to reach 15 mg quickly. The four-week minimum between dose increases is a floor; there is no ceiling on how long you may remain at any given dose before deciding whether to move up, per Zepbound prescribing information, Section 2.1.
Can I stay on 5 mg Zepbound forever?
Yes. 5 mg is an FDA-approved maintenance dose for chronic weight management. In SURMOUNT-1 in NEJM 2022, it produced −15.0% mean body weight loss at 72 weeks, a clinically significant and durable outcome. If you are meeting your weight-management goals at 5 mg with good tolerability, there is no clinical requirement to escalate. Note that 5 mg is not approved as an OSA maintenance dose; patients using Zepbound for sleep apnea must reach at least 10 mg.
What is the Zepbound dosage for sleep apnea versus weight loss?
The titration sequence is identical for both indications, start at 2.5 mg, advance every ≥4 weeks in 2.5 mg steps. The difference is in maintenance. For weight loss, maintenance is permitted at 5 mg, 10 mg, or 15 mg. For OSA, per Zepbound prescribing information, Section 2.2, the approved maintenance doses are 10 mg or 15 mg only, 5 mg is not an approved maintenance dose for OSA. Patients prescribed Zepbound for sleep apnea who tolerate 5 mg well must still continue titrating to 10 mg.
What happens if I miss a Zepbound dose?
Per Zepbound prescribing information, Section 2.3: if 4 days (96 hours) or fewer have passed since your scheduled injection, administer the missed dose as soon as possible and resume your regular weekly schedule. If more than 4 days have passed, skip the missed dose entirely and take your next injection on your usual day. Never take two doses in the same week to compensate for a missed one.
Is the 2.5 mg dose effective for weight loss?
No. 2.5 mg is not FDA-approved as a maintenance dose, and it is not expected to produce clinically meaningful weight loss. It is a tolerability-initiation step only. The SURMOUNT-1 trial tested 5 mg, 10 mg, and 15 mg maintenance doses; 2.5 mg was not evaluated as a maintenance option. Clinically significant weight loss, averaging −15.0% of body weight, begins at the 5 mg maintenance level, per SURMOUNT-1 in NEJM 2022.
This article is for informational purposes only and does not constitute medical advice. Dosing decisions — including initiation, escalation, and hold, are made by your prescribing clinician. Prescribing information, pricing, and regulatory status reflect data as of April 2026 and are subject to change. WeightLossInjections.com editorial team verifies content quarterly; last verified April 2026.