
Zepbound Nausea Timeline Across Three Phases
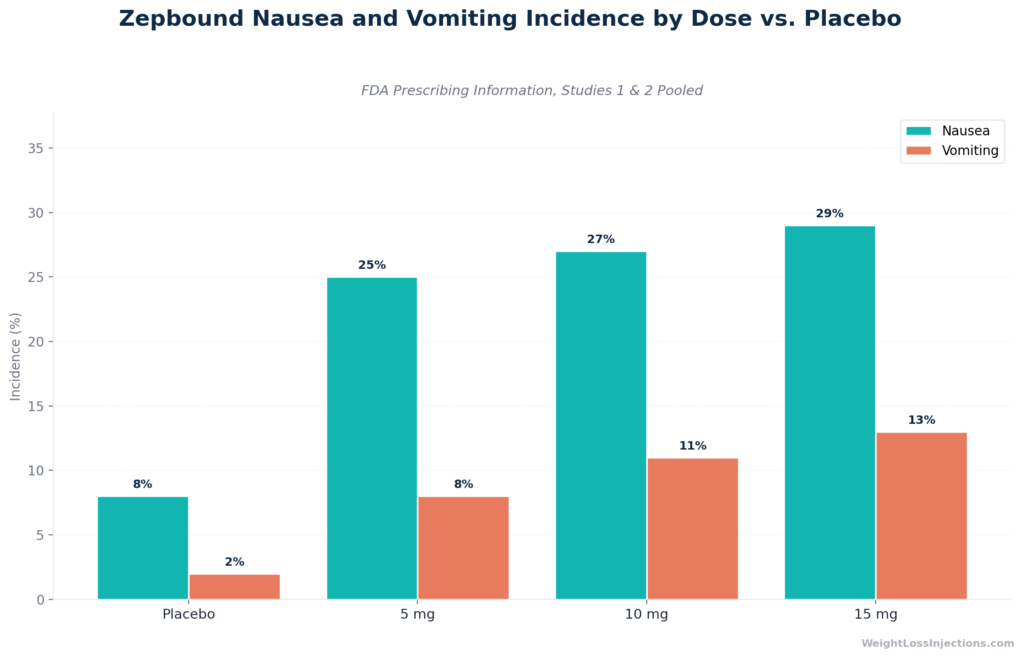
Nausea is the most common single adverse effect of Zepbound, affecting 25% of patients on 5 mg, 27% on 10 mg, and 29% on 15 mg in the FDA prescribing information, versus 8% on placebo. For most patients, it is mild-to-moderate, peaks 2–5 days after each injection, and resolves within 1–2 weeks. It recurs with every dose escalation, but declines substantially after 8–12 weeks on a stable dose.
Nausea alone is rarely a reason to stop treatment; it is almost always manageable with dietary strategies, injection timing, and, when needed, a slower titration schedule.
Safety notice: This article is for educational purposes only. It does not constitute medical advice. Severe or persistent nausea, particularly when accompanied by upper abdominal pain, vomiting that prevents fluid intake, or signs of dehydration, requires prompt evaluation by a licensed healthcare provider.
How Common Is Zepbound Nausea? What the FDA Data Shows
Most published discussions of Zepbound nausea quote approximate or rounded figures. The table below reproduces the exact incidence rates from Table 1 of the Zepbound FDA prescribing information, drawn from the pooled placebo-controlled SURMOUNT Studies 1 and 2.
Nausea and Vomiting Rates by Dose (FDA Label, Studies 1 & 2 Pooled)
| Adverse Reaction | Placebo (N=958) | Zepbound 5 mg (N=630) | Zepbound 10 mg (N=948) | Zepbound 15 mg (N=941) |
|---|---|---|---|---|
| Nausea | 8% | 25% | 27% | 29% |
| Vomiting | 2% | 8% | 11% | 13% |
| Diarrhea | 8% | 19% | 21% | 23% |
| Constipation | 5% | 17% | 14% | 11% |
Source: Zepbound prescribing information, Table 1
Note: The brief’s nausea figures by dose are 25% / 27% / 29% as reproduced directly from the FDA label above. A few observations are worth underscoring.
First, the placebo nausea rate is 8%, meaning roughly one in twelve patients experiences nausea independent of the drug. The drug-attributable excess is approximately 17–21 percentage points across the three maintenance doses. Second, nausea rises incrementally with dose, while constipation actually declines, suggesting these GI effects arise from partially different mechanisms. Third, vomiting rates are substantially lower than nausea rates, confirming that most patients feel nauseated without vomiting, which is clinically meaningful: the symptom is unpleasant but less disruptive than frank emesis.
Looking at the broader GI picture, gastrointestinal adverse events of any type affected 56% of pooled Zepbound patients versus 30% on placebo, per the Zepbound prescribing information. Severe GI adverse events, those requiring medical intervention or causing treatment discontinuation, occurred in 1.7% of 5 mg patients, 2.5% of 10 mg patients, and 3.1% of 15 mg patients, versus 1.0% on placebo. The serious event rate is low, but the overall GI burden is real and concentrated in the titration phase.
Good News: Nausea Is Largely Mild and Front-Loaded
The numbers in the table above reflect cumulative rates across the full 72-week SURMOUNT-1 trial duration, they do not mean that one-quarter to one-third of patients feel nauseated every week throughout treatment. In the SURMOUNT-1 trial published in NEJM, gastrointestinal adverse events were heavily concentrated in the first four weeks of treatment and at each subsequent dose escalation step. After 8–12 weeks on a stable dose, GI symptom rates declined substantially, and most patients on long-term treatment no longer listed nausea as a meaningful complaint.
The 2.5 mg starting dose is a deliberate design choice. Per the Zepbound prescribing information, 2.5 mg is a tolerability step only, not an approved maintenance dose, specifically intended to allow the GI tract to acclimate before reaching therapeutic doses. The slow four-week-minimum titration interval between every dose increase serves the same purpose. Nausea on Zepbound is expected, but it is not permanent.
Why Does Zepbound Cause Nausea? The Dual-Receptor Mechanism
Competitors often reduce Zepbound nausea to a single sentence: “GLP-1 slows gastric emptying.” That is accurate but incomplete. Tirzepatide’s nausea mechanism involves at least three interacting pathways, all documented in the Zepbound prescribing information.
Gastric Emptying Delay: The Primary Driver
Tirzepatide activates both the GLP-1 receptor (GLP-1R) and the GIP receptor (GIPR), making it the first approved dual GIP/GLP-1 receptor agonist. Both receptor pathways contribute to slowing the rate at which food leaves the stomach (Zepbound prescribing information). When gastric emptying is delayed, food remains in the stomach longer than normal, producing prolonged gastric distension. That mechanical stretch, combined with the hormonal signaling from incompletely emptied stomach contents, generates nausea and early satiety.
This effect is dose-dependent: higher doses slow gastric emptying more aggressively, which explains, at least in part, why nausea rates increase from 25% at 5 mg to 29% at 15 mg. The effect is also most pronounced during the first weeks of treatment at any given dose, before the gut partially adapts.
Central Chemoreceptor Trigger Zone (CTZ) Activation
GLP-1 receptors are expressed not only in the gut but also in the brainstem, specifically the area postrema, the chemoreceptor trigger zone (CTZ) that directly stimulates the vomiting center. When tirzepatide activates these central GLP-1 receptors, it can generate nausea and the impulse to vomit independently of what is happening in the stomach (Zepbound prescribing information). This is why some patients experience nausea even on an empty stomach, and why nausea can begin within hours of an injection rather than only after eating.
Over time, the brainstem receptors undergo partial adaptation to sustained GLP-1 receptor stimulation, which is a key reason nausea diminishes after weeks on a stable dose.
GIP Receptor Contribution: What Makes Tirzepatide Different
Unlike semaglutide (which acts solely on GLP-1R), tirzepatide also activates GIPR, the glucose-dependent insulinotropic polypeptide receptor. GIPR is expressed in adipose tissue, the gut, and the brain. Per the Zepbound prescribing information, GIPR activation contributes to insulin secretion, suppresses glucagon, and reduces adipogenesis via adipose tissue GIPR.
The dual agonism is also why tirzepatide produces superior weight loss compared with GLP-1–only agents: the GIP receptor pathway adds a distinct metabolic effect. The trade-off is that engaging a second receptor with GI and central nervous system distribution adds a second nausea-generating pathway. This does not necessarily mean tirzepatide causes more nausea than GLP-1–only agents in head-to-head comparisons, but it does mean the mechanism is more complex, and that strategies targeting only one pathway may not fully resolve symptoms.
Appetite Suppression as Perceived Nausea
A subtler mechanism: GLP-1R activation in the hypothalamus generates strong satiety signaling that reduces appetite. Some patients interpret this profound fullness or absence of hunger as nausea, a sense of queasiness that is neurologically adjacent to satiety but not always driven by gastric distension. This effect diminishes with adaptation and helps explain why some patients report feeling “sick” even after very small meals or on an empty stomach early in treatment.
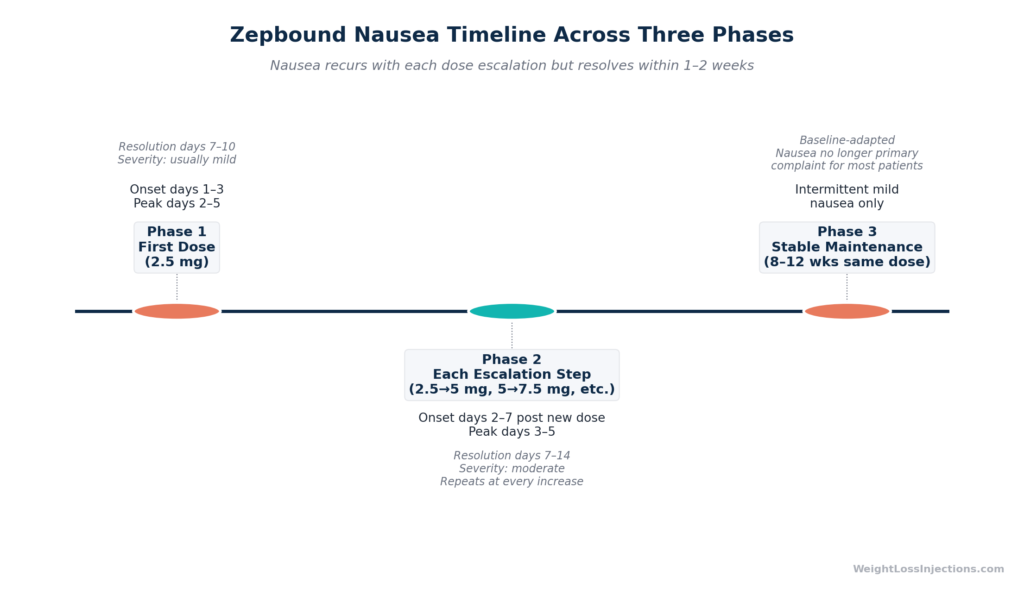
Zepbound Nausea Timeline: Three Distinct Phases
Nausea on Zepbound does not follow a simple course. Understanding its three-phase pattern allows patients to anticipate what is coming, recognize normal from concerning, and make better decisions about titration.
Phase 1: First Dose (Week 1, 2.5 mg)
The 2.5 mg starting dose is designed to minimize nausea, but first exposures still produce a response in some patients. Nausea typically begins on days 1–3 post-injection and peaks around days 2–5, when tirzepatide reaches maximum plasma concentration (Tmax is 8–72 hours after subcutaneous injection, per the Zepbound prescribing information). For most patients at the starting dose, nausea is mild and resolves within 7–10 days as the body begins to adapt.
This phase is often the least severe in absolute terms, the dose is low, and it is the body’s first exposure to the mechanism.
Phase 2: Each Dose Escalation Step
Every dose increase triggers a mini-recurrence of nausea. This is the phase that surprises patients most: they adapted to 2.5 mg without incident, but increasing to 5 mg brings nausea back. The pattern repeats at every step — 5 → 7.5 mg, 7.5 → 10 mg, and so on through the minimum 20-week titration schedule to reach 15 mg (Zepbound prescribing information).
Escalation nausea typically begins within 2–7 days of the new dose and resolves within 1–2 weeks. Peak intensity at escalation is often more significant than Phase 1 because the absolute dose is higher. Per SURMOUNT-1 in NEJM, GI adverse events were concentrated not only in the first four weeks but also at each subsequent escalation step, making this a recurring feature of the titration journey, not a one-time hurdle.
Practical implication: Do not assume that tolerating one dose well means all future escalations will be similarly smooth. The body re-adapts at each new exposure level.
Phase 3: Stable Dose Maintenance
After 8–12 weeks on a consistent dose without escalation, nausea rates decline substantially. As documented in SURMOUNT-1, GI adverse event rates in the trial dropped significantly after the escalation period ended. Most patients on long-term stable treatment report that nausea is no longer a significant day-to-day issue, though occasional mild nausea, particularly after large or high-fat meals, may persist sporadically.
The key insight: if a patient is told their nausea “usually goes away,” the answer is qualified by dose stability. Nausea does go away, but it can come back with each escalation. Knowing this in advance reduces distress when it happens.
8 Evidence-Based Strategies to Reduce Zepbound Nausea
The following strategies are grounded in the mechanism of tirzepatide-associated nausea and consistent with guidance in the Zepbound prescribing information and Zepbound.lilly.com How to Use page.
1. Eat Smaller, More Frequent Meals
Large meals stress an already-slowed gastric emptying system. Eating 4–6 small meals per day rather than 3 large ones reduces the amount of food in the stomach at any given time, directly limiting the gastric distension that drives nausea. The practical rule: stop eating at 70–80% fullness, because tirzepatide’s gastric emptying delay means that fullness will continue to build for 20–30 minutes after you stop eating. What feels like “just enough” at the table can feel like overeating an hour later.
2. Avoid High-Fat and Fried Foods
Fat is the most slowly digested macronutrient. In a stomach already slowed by tirzepatide, high-fat meals compound the delay dramatically, prolonging distension and worsening nausea. The Zepbound prescribing information specifically notes that nausea can be reduced by avoiding high-fat meals. This does not mean eliminating healthy fats permanently, but on the days surrounding an injection, particularly days 2–5 when nausea peaks, fried foods, heavy sauces, full-fat dairy, and fatty meats are best minimized.
For a comprehensive dietary guide to what to eat and avoid on Zepbound, see our article on foods to avoid on Zepbound.
3. Space Fluids Away from Meals
Drinking large amounts immediately before, during, or after meals adds volume to a stomach that is emptying slowly. The result: increased gastric distension, worsened nausea, and early satiety that disrupts nutritional intake. A practical protocol: avoid drinking more than a few sips for 30 minutes before and 30–60 minutes after meals. Stay well hydrated throughout the day in small, consistent increments, sipping water between meals rather than gulping during them.
4. Choose Injection Timing Strategically
Nausea peaks approximately 2–5 days after injection but can begin within 24–48 hours, during or shortly after Tmax. Some patients find that injecting in the evening means the initial nausea occurs during overnight hours, when they are asleep and eating minimally. Others prefer morning injections on a day they can take it easy. Neither approach is formally endorsed by the Zepbound prescribing information, the label states Zepbound can be taken at any time of day, with or without food, but consistency in weekly timing reduces variability in the nausea experience.
5. Eat Bland Foods During Peak Nausea Days
During the 2–5 days post-injection when nausea peaks, defaulting to low-stimulation foods reduces symptom severity. Toast, plain crackers, plain oatmeal, bananas, and broth are classic examples, low-fat, low-fiber, easy to digest, and unlikely to generate additional GI distress. Avoid spicy foods, acidic foods (citrus, tomato-based), and very sweet or high-sugar items during this window. The BRAT approach (bananas, rice, applesauce, toast) developed for GI illness applies here: bland reduces the baseline GI load when the gut is already taxed.
6. Stay Upright After Eating
Tirzepatide’s gastric emptying delay means food sits in the stomach longer than normal. Lying down with a full stomach increases the risk of gastroesophageal reflux, which compounds nausea, particularly since gastroesophageal reflux disease (GERD) is listed as a reported adverse event in the FDA-approved Zepbound label. Remain upright for at least 30–60 minutes after eating. A gentle 15–20 minute walk after meals aids gastric motility and can meaningfully reduce post-meal nausea.
7. Try Ginger
Ginger (Zingiber officinale) has demonstrated anti-nausea properties across multiple mechanisms, including 5-HT3 receptor antagonism, the same receptor class targeted by prescription antiemetics like ondansetron. Multiple systematic reviews support its efficacy for chemotherapy-induced and pregnancy-related nausea. While no large randomized trial has been conducted specifically for GLP-1–associated nausea, the mechanistic overlap is plausible. Options include ginger tea brewed from fresh or dried root, ginger chews, ginger capsules (250–1,000 mg doses), or flat ginger ale made with real ginger extract. Ginger is generally safe and inexpensive, making it a reasonable first-line adjunct during peak nausea days.
8. Discuss Antiemetic Options with Your Provider
For patients whose nausea is severe enough to interfere with daily function or adequate nutrition, prescription antiemetics are available and appropriate. Providers may prescribe ondansetron (Zofran), promethazine, or other antiemetics for use during the first days post-injection. Over-the-counter options include meclizine (Dramamine) and, with provider guidance, bismuth subsalicylate (Pepto-Bismol).
Acupressure wristbands targeting the P6 (Neiguan) point have also shown benefit: a 2025 study indexed in PMC (PMC12137197) found that acupressure wristbands provided nausea relief within 20 minutes for GLP-1–associated nausea, with no drug interactions or adverse effects. They are inexpensive and worth trying as a first step before medication.
The critical point: do not stop Zepbound without provider consultation because of nausea alone. Per SURMOUNT-4 published in JAMA, patients who discontinued tirzepatide regained an average of +14.0% body weight in the 52 weeks following withdrawal. Nausea is almost always manageable with the strategies above; stopping treatment to avoid nausea trades a temporary discomfort for long-term weight regain.
When to Slow Your Titration (or Stay at the Current Dose)
The titration schedule in the Zepbound prescribing information specifies a minimum of four weeks between each dose increase. The operative word is minimum. There is no clinical requirement to escalate on schedule, and staying at a lower dose for longer is a legitimate, provider-guided strategy for patients with significant escalation nausea.
Indications for discussing a delayed titration:
- Nausea is still significantly impairing daily function — affecting sleep, work, or the ability to eat adequate nutrition — at the end of week 4 on the current dose
- Nausea at week 4 has not followed the expected pattern of improvement from the peak at days 2–5
- Prior dose escalation triggered nausea that lasted more than two weeks
What adjusted titration looks like in practice: Staying at 2.5 mg for 8 weeks instead of 4 weeks before moving to 5 mg is clinically acceptable and well within the label’s guidance. A provider might also recommend temporarily stepping back from 5 mg to 2.5 mg if escalation nausea is severe and persistent. These are not treatment failures — they are appropriate individualization of a protocol designed with flexibility.
The broader principle: the titration schedule exists to guide typical tolerability. Patients with significant GI sensitivity may need more time between steps. Working with a provider who actively monitors side effects and adjusts the schedule accordingly produces meaningfully better outcomes than rigidly advancing on the calendar regardless of tolerability.
When Nausea Is a Warning Sign: Red Flags to Know
Most Zepbound nausea is physiologically benign, unpleasant but not dangerous. But nausea can also be the presenting symptom of a serious underlying complication. The following patterns require immediate attention.
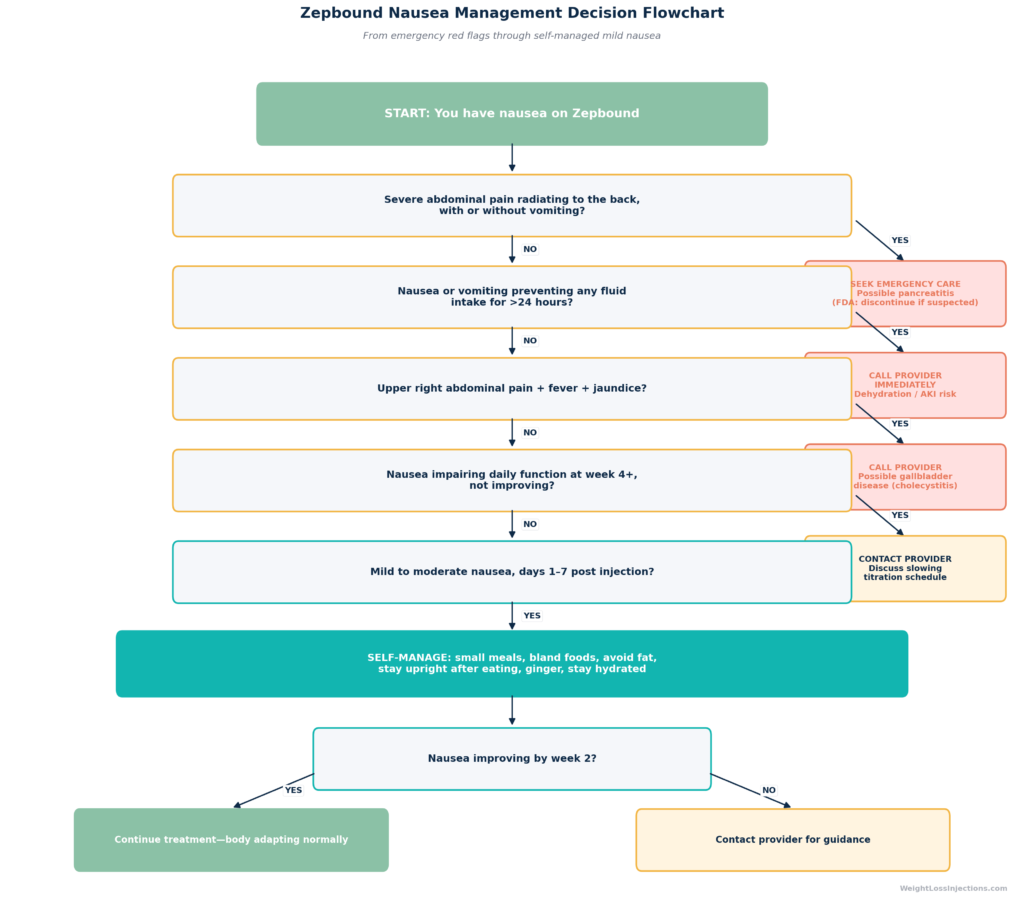
Zepbound Nausea Decision Flowchart
Possible Pancreatitis: Seek Emergency Care
Nausea accompanied by severe abdominal pain that radiates to the back, with or without vomiting, is the hallmark presentation of acute pancreatitis. This is not typical Zepbound nausea. Per the Zepbound prescribing information Warnings and Precautions section, pancreatitis has been reported in patients treated with tirzepatide. The FDA label states explicitly: discontinue Zepbound if pancreatitis is suspected. Zepbound has not been studied in patients with a history of pancreatitis. If severe mid-to-upper abdominal pain with back radiation occurs, stop the next scheduled dose and seek emergency evaluation, do not wait for improvement.
Possible Gallbladder Disease
Cholelithiasis (gallstones) and cholecystitis (gallbladder inflammation) have both been reported with Zepbound, consistent with GLP-1–class effects on bile composition and gallbladder contractility (Zepbound prescribing information). The presenting symptom is typically nausea combined with pain in the upper right abdomen (below the right rib cage), which may radiate to the right shoulder. Fever and jaundice (yellowing of the skin or eyes) indicate more advanced gallbladder disease. Any of these combinations requires provider evaluation, not self-management.
Dehydration and Acute Kidney Injury Risk
If nausea leads to vomiting or diarrhea severe enough to prevent adequate fluid intake for more than 24 hours, dehydration becomes a clinical concern. Per the Zepbound prescribing information, acute kidney injury (AKI) has been reported in patients treated with tirzepatide, the mechanism is GI-mediated volume depletion that reduces renal perfusion. The FDA label instructs providers to advise patients to take precautions to avoid fluid depletion and to monitor renal function when GI adverse reactions occur.
Signs that require same-day provider contact:
- Dark yellow or amber urine (concentrated urine indicating volume depletion)
- Substantially reduced urine output — fewer than three voids in 24 hours
- Dizziness or lightheadedness on standing
- Inability to keep any fluids down for more than 12 hours
- Dry mouth, rapid heart rate, or pronounced weakness
Patients on concurrent diuretics, ACE inhibitors, ARBs, or NSAIDs face elevated AKI risk at lower levels of fluid loss and should have a lower threshold for contacting their provider.
When to Consider Stopping Zepbound
Only with provider guidance. Nausea alone, absent the red flags above, is rarely sufficient clinical reason to discontinue Zepbound. The benefit-risk calculation almost always favors continuing with dose adjustment over stopping entirely, particularly given the documented weight regain after discontinuation. Per SURMOUNT-4 in JAMA, patients who stopped tirzepatide after initial weight loss regained a mean of +14.0% body weight in the subsequent 52 weeks, while those who continued tirzepatide lost an additional −5.5%, a 19.4 percentage point treatment difference. Obesity is a chronic condition requiring long-term treatment, and nausea management is a solvable problem.
Our take at WeightLossInjections.com: Nausea is Zepbound’s most common side effect and, in clinical practice, its most talked-about one. The conversations we have with patients reveal a consistent pattern: nausea was expected in the abstract, but the escalation recurrence is what catches people off guard. They tolerated 2.5 mg well, felt confident about the process, escalated to 5 mg, and the nausea returned. Understanding that this is not a signal of something going wrong, but rather the expected pharmacological response to a higher dose that requires its own adaptation period, is genuinely useful. The eight strategies in this article are not hypothetical, they reflect what works based on the mechanism and clinical experience. The most effective predictor of which patients manage Zepbound nausea well is not their innate GI sensitivity; it is whether they had a plan before the first injection. Patients who know which foods to avoid, who understand the timing of peak nausea, and who have talked with their provider about the titration pace are consistently better positioned than those improvising after the fact. If you are considering Zepbound and want to start with a provider who actively manages side effects and individualizes your titration schedule, WeightLossInjections.com connects you with licensed telehealth providers who treat nausea management as part of the treatment protocol, not an afterthought. Telehealth visits for [service detail] run [$X/month] and include dose adjustment support throughout the titration phase.
Frequently Asked Questions
How long does Zepbound nausea last?
It depends on which phase you are in. First-dose nausea at 2.5 mg typically peaks on days 2–5 and resolves within 7–10 days for most patients. With each dose escalation, nausea recurs and usually resolves within 1–2 weeks per the Zepbound prescribing information. After 8–12 weeks on a stable maintenance dose without escalation, consistent with what was seen in SURMOUNT-1 in NEJM, nausea rates decline substantially and most patients report it is no longer a daily issue. Nausea that persists beyond two weeks on a stable dose without improvement warrants a provider conversation.
Does Zepbound nausea get better with each dose?
Not linearly. Nausea does improve after the body adapts to each dose level, but it returns when the dose increases. The pattern is: nausea at first exposure → adaptation over 1–2 weeks → nausea returns at the next escalation step → adaptation again. By the time a patient reaches their maintenance dose and stays there, the cycle ends and nausea typically subsides to a background level. The full titration to 15 mg requires a minimum of 20 weeks per the Zepbound prescribing information, meaning this escalation-adaptation cycle can repeat up to five times.
What can I take for nausea while on Zepbound?
Start with non-pharmacological strategies: small bland meals, avoiding high-fat foods, staying upright after eating, and ginger (tea, chews, or capsules). For short-term relief, acupressure wristbands targeting the P6 point have shown benefit in GLP-1–associated nausea (PMC12137197, 2025). If nausea is severe or interfering with nutrition, discuss antiemetic options with your prescribing provider, ondansetron (Zofran) is commonly prescribed off-label for this purpose, and OTC meclizine (Dramamine) may provide relief. Do not take any new medication without consulting your provider first, as drug interactions and underlying conditions matter.
Is Zepbound nausea a sign it’s working?
Nausea reflects tirzepatide’s pharmacological effects on gastric emptying and central appetite signaling, both of which contribute to weight loss. In that sense, nausea and weight loss share a common cause. However, nausea itself is not required for the drug to work, and patients who experience minimal nausea still achieve substantial weight loss in clinical trials. The Zepbound prescribing information does not characterize nausea as a marker of efficacy. Some patients with very little nausea achieve excellent results; some patients with significant nausea do not. The presence or absence of nausea should not be used to gauge whether treatment is “working.”
Should I stop Zepbound if I’m nauseous?
Not without consulting your provider. Nausea alone is almost never a sufficient reason to discontinue, because it is expected, temporary, and manageable with dose adjustment and dietary strategies. The consequences of stopping are significant: per SURMOUNT-4 in JAMA, patients who discontinued tirzepatide regained an average of +14.0% of body weight in 52 weeks. If nausea is severe, persistent, or affecting your quality of life significantly, the right response is to contact your provider to discuss slowing the titration schedule or using antiemetics, not to stop the medication unilaterally.
What foods make Zepbound nausea worse?
High-fat and fried foods top the list, fat is the slowest macronutrient to digest and compounds the gastric emptying delay caused by tirzepatide. The Zepbound prescribing information specifically advises avoiding high-fat meals to reduce nausea. Beyond fat, spicy foods, highly acidic foods (citrus, tomato-based dishes), large portions of any type, carbonated beverages, and high-sugar foods can all worsen GI symptoms in patients with delayed gastric emptying. Alcohol is an additional irritant that can worsen nausea and dehydration simultaneously. During the peak nausea window of days 2–5 post-injection, sticking to bland, low-fat, easily digestible foods meaningfully reduces symptom severity for most patients. For a detailed dietary guide, see our article on foods to avoid on Zepbound.
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. Always consult your licensed healthcare provider before making any changes to your medication regimen.