
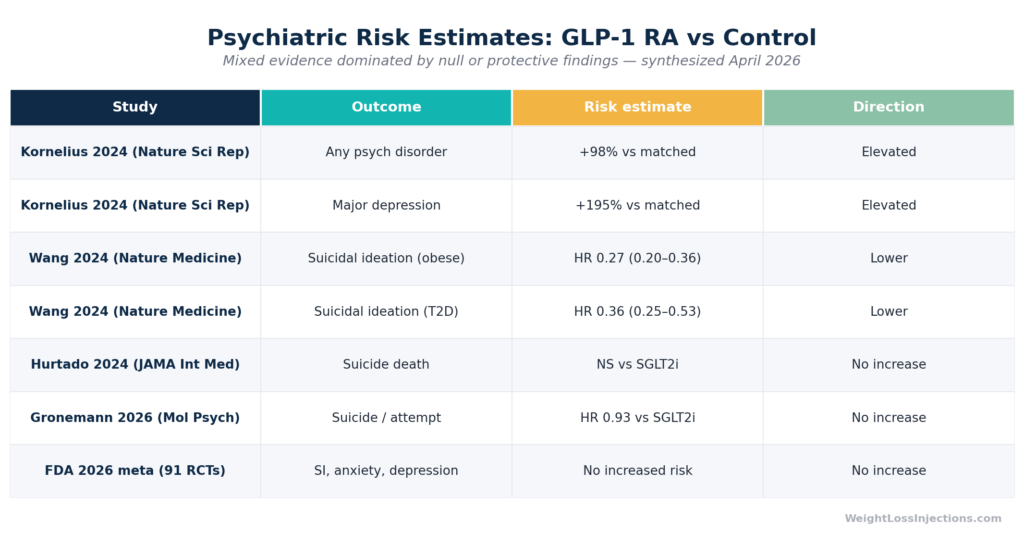
Hero comparison table of Psychiatric Hazard Ratios: GLP-1 vs Control Across Key Studies
Reports of mood changes on Ozempic (semaglutide) are real, documented in pharmacovigilance databases and case series, and serious enough to warrant proactive monitoring, but the overall body of evidence, culminating in an FDA meta-analysis of 107,910 patients published in January 2026, does not support a causal link between semaglutide and depression, anxiety, or suicidal ideation. One large 2024 observational study in obesity patients found substantially elevated psychiatric event rates in GLP-1 users; multiple other large cohort studies found no increased risk or lower risk.
The honest answer is that the evidence is conflicting, the populations studied differ importantly, and confounding by pre-existing psychiatric comorbidity remains difficult to fully eliminate. What matters practically: screen before starting, log mood weekly, and know exactly when to call your provider or go to the emergency room.
Safety notice: This article is for educational purposes only and does not constitute medical advice. If you are experiencing depression, thoughts of self-harm, or a psychiatric emergency, stop reading and call or text 988 (Suicide and Crisis Lifeline) or go to your nearest emergency department immediately.
What Are Ozempic Mental Side Effects?
Ozempic (semaglutide injection) was approved by the FDA in December 2017 for glycemic control in adults with type 2 diabetes (NDA 209637). Its well-known side effects are gastrointestinal, nausea, vomiting, diarrhea, but a separate category of reported effects involves mood, cognition, and behavior.
Patients and clinicians have described a loose cluster of psychiatric symptoms: diminished pleasure in activities, emotional flatness, increased irritability or anxiety, low motivation, and, in rarer and more serious cases, depressive episodes and suicidal thinking. Social media and mainstream press have wrapped this cluster under the informal label “Ozempic personality” — a term that has no clinical definition but captures something patients say they experience.
Per the Ozempic prescribing information (2025), psychiatric adverse events are not listed among the warnings, precautions, or common adverse reactions. Specifically, Section 5 (Warnings and Precautions), Section 6.1 (Clinical Trials Experience), and Section 6.2 (Postmarketing Experience) of the current Ozempic PI contain no language about depression, anxiety, suicidal ideation, or mood disorders, a point that matters clinically and distinguishes Ozempic from some of its weight-management-indication counterparts.
Wegovy (semaglutide 2.4 mg, approved for chronic weight management) previously carried a class-effect warning for suicidal behavior and ideation — language added after a small number of events were observed in clinical trials of liraglutide and semaglutide for weight management. In January 2026, following a comprehensive evidence review, the FDA requested removal of that warning from Wegovy, Saxenda (liraglutide), and Zepbound (tirzepatide) — reflecting its conclusion that no causal relationship with suicidal ideation or behavior has been established.
Common Reported Symptoms
Depression and Low Mood
Clinical depression involves persistent low mood, loss of interest in previously enjoyable activities (anhedonia), fatigue, impaired concentration, psychomotor slowing, and in severe cases, feelings of hopelessness or worthlessness. These symptoms have been reported in pharmacovigilance databases in patients using semaglutide, though the overall rate remains low relative to total user numbers.
A 2024 analysis of the EudraVigilance spontaneous reporting database, covering 31,444 adverse event reports for GLP-1 receptor agonists, found that psychiatric adverse events constituted just 1.18% of all reports (372 cases, 481 events). Among those 372 psychiatric cases, depression was the most common single preferred term, accounting for 50.3% of psychiatric reports (187 cases total, with 117 attributed to semaglutide specifically) (Tobaiqy & Elkout, Pharmaceuticals, 2024). These are spontaneous reports, not denominator-adjusted incidence rates; they establish that depression is reported but cannot quantify population-level risk.
Two case reports published in Frontiers in Psychiatry (August 2023) described patients who developed depressive symptoms approximately one month after starting semaglutide, with symptoms resolving within one to two weeks of discontinuation. One patient had no prior psychiatric history; the other had a history of recurrent major depression that appeared to relapse. Both cases resolved after stopping the medication, though the authors cautioned that confounding factors could not be excluded and that the temporal association alone does not establish causation (Li et al., Front. Psychiatry, 2023).
Anxiety and Irritability: The “Ozempic Personality” Phenomenon
The “Ozempic personality” concept gained traction in 2024 through social media posts and media coverage in outlets including the New York Post and Daily Mail, describing users who felt emotionally flat, irritable, or less engaged with previously pleasurable activities — a pattern clinicians recognize as consistent with anhedonia. The Healthline reporting on this phenomenon quoted experts who disputed the label while acknowledging patient experiences; the most common reported features were increased irritability, emotional numbing, lower motivation, and reduced libido.
Anxiety was the second most common psychiatric preferred term in the EudraVigilance pharmacovigilance database, accounting for 38.7% of psychiatric reports (144 cases; 71 attributed to semaglutide) (Tobaiqy & Elkout, 2024). Again, these are raw reports from a drug-safety monitoring database, not controlled incidence data.
Biologically, GLP-1 receptors are expressed in mood-relevant brain regions, the amygdala, hippocampus, hypothalamus, and nucleus accumbens, and influence dopamine signaling in the ventral tegmental area (VTA), the hub of the brain’s reward circuit (Frontiers in Pharmacology, 2020). Pharmacological activation of GLP-1 receptors reduces food-related reward signaling and has been shown to blunt responses to alcohol and nicotine in animal models. The working hypothesis for “Ozempic personality” is that the same dopaminergic dampening that reduces food cravings may, in susceptible individuals, broadly reduce reward responsiveness, producing emotional flattening, not a true personality change (PMC Neuroscience Applied, 2025). This mechanism remains hypothetical; human trial data have not established it as causal.
An equally plausible explanation: rapid caloric restriction and weight loss are themselves physiologically stressful, activate the HPA axis, and alter sex hormone levels, all of which can produce mood changes independent of semaglutide’s direct CNS effects. Disentangling drug effects from the psychological and physiological impact of rapid weight loss is a core methodological challenge in this literature.
Suicidal Ideation and Thoughts of Self-Harm
Suicidal ideation (SI) is the most serious reported psychiatric adverse event in this space and the one that triggered regulatory review. In the EudraVigilance pharmacovigilance database analysis, suicidal ideation was reported in 73 of 372 psychiatric cases (19.6%): 40 cases with semaglutide, 29 with liraglutide, 4 with tirzepatide (Tobaiqy & Elkout, 2024). Suicide attempts numbered 12 cases (5 with semaglutide), and there were 4 completed suicides across the database (all with liraglutide). These figures represent a raw count across years of post-marketing surveillance for drugs used by millions of people globally; the absolute rates are very low.
An August 2024 disproportionality analysis based on the WHO global pharmacovigilance database (36 million adverse drug reaction reports across 140 countries) found that semaglutide showed a statistically significant reporting odds ratio of 1.45 (95% CI not fully reported) for suicidal ideation compared with all other medications — with an amplified signal (OR 4.45) in patients also taking antidepressants (The Pharmaceutical Journal, August 2024). Disproportionality analyses detect reporting signals, not absolute risk, and are subject to confounding by indication — patients taking antidepressants already carry elevated baseline suicide risk, independent of semaglutide.
Scientific Evidence: What the Studies Actually Show
This is the section where honest synthesis matters most. The studies do not all point the same direction, and the differences in findings are explained largely by differences in study populations, comparator groups, and methodology.
Studies Reporting Elevated Risk
The most prominent risk-signal study was published in Nature Scientific Reports in October 2024 (PMID: s41598-024-75965-2). Kornelius and colleagues conducted a large community-based cohort study using post-marketing data from January 2015 to December 2023, propensity-matching 162,253 patients with obesity — 81,126 who were prescribed a GLP-1 receptor agonist (liraglutide or semaglutide) and 81,127 matched controls who were not. In this obesity cohort, GLP-1 RA users had substantially elevated event rates across all psychiatric outcomes: any psychiatric disorder (+98%), major depression (+195%), anxiety (+108%), and suicidal behavior (+106%).
Several important caveats apply. The study population was specifically patients with obesity, a group that carries substantially elevated baseline risk for depression, anxiety, and suicidal ideation — rates that are 2–3 times higher than the general population. Propensity score matching adjusts for observable confounders, but cannot account for unmeasured psychiatric history, antidepressant use patterns, or differential healthcare surveillance (patients prescribed GLP-1 RAs may simply be seen more often, generating more recorded psychiatric diagnoses). The authors appropriately note these limitations and frame findings as associational.
Studies Reporting No Increased or Lower Risk
A large retrospective cohort study published in Nature Medicine (January 2024) — using nationwide electronic health records from the TriNetX Analytics Network — examined 240,618 patients with overweight or obesity and 1,589,855 patients with type 2 diabetes. Among patients with overweight or obesity, semaglutide was associated with a significantly lower risk of incident suicidal ideation compared with non-GLP-1 anti-obesity medications (HR 0.27, 95% CI 0.20–0.36). For recurrent suicidal ideation, the hazard ratio was 0.44 (95% CI 0.32–0.60). In the larger T2DM cohort, incident suicidal ideation was also lower in semaglutide users (HR 0.36, 95% CI 0.25–0.53). These associations remained consistent across sex, age group, and ethnicity subgroups. The authors cautioned that the findings are observational and reverse causality — where unmeasured suicidal ideation influences which medication a provider selects — cannot be excluded.
A second 2024 binational cohort study published in JAMA Internal Medicine — which followed predominantly T2DM patients in two countries — found no statistically significant increased risk of suicide death comparing GLP-1 RA users to SGLT2 inhibitor users, with an upper confidence interval compatible with an absolute risk increase of no more than 0.16 suicide deaths per 1,000 person-years. There was a slightly lower risk of self-harm and no significant association with incident depression or anxiety-related disorders.
A 2026 nationwide Danish register study in Molecular Psychiatry (Nature Portfolio) found that GLP-1 RA users had no increased hazard of suicide or suicide attempts versus SGLT2 inhibitor users (HR 0.93, 95% CI 0.57–1.52), and had a lower hazard versus DPP-4 inhibitor users (HR 0.58, 95% CI 0.37–0.91). In a self-controlled case series design, GLP-1 RA use was associated with a lower incidence rate ratio for suicide or suicide attempts during both the first year (IRR 0.45, 95% CI 0.10–0.50) and months 13–24 after treatment initiation.
A 2025 systematic review and meta-analysis in Diabetes/Metabolism Research and Reviews pooling four studies found no statistically significant association between GLP-1 RA use and suicidal ideation or behavior (RR 0.568, 95% CI 0.077–4.205), though the authors noted high heterogeneity (I² = 98%) warranting cautious interpretation.
The FDA’s January 2026 Determination
In January 2026, the FDA completed its most comprehensive review to date. The agency conducted a meta-analysis of 91 placebo-controlled clinical trials spanning GLP-1 RA development programs, totaling 107,910 patients — 60,338 treated with a GLP-1 RA and 47,572 treated with placebo. The results showed no increased risk of suicidal ideation or behavior, and no increased risk of anxiety, depression, irritability, or psychosis. The FDA also analyzed a retrospective cohort of more than 2 million users and reviewed published observational and pooled studies.
The agency’s formal conclusion: “the totality of these studies does not support a causal relationship between the use of GLP-1 RAs and the occurrence of suicidal ideation and behavior” (Medscape, January 14, 2026). On the basis of this review, the FDA requested removal of the existing suicidal ideation/behavior warning from Wegovy, Saxenda, and Zepbound labeling — the labels that had carried such language — and confirmed that the Ozempic prescribing information requires no change because it never included a psychiatric warning.
The European Medicines Agency reached the same conclusion following its own parallel analysis (GoodRx, citing EMA PRAC meeting, April 2024).
Emerging evidence is now moving beyond simply ruling out harm. A 2026 national cohort study cited by the Psychopharmacology Institute found that semaglutide was associated with a 42% lower risk of worsening mental illness (including depression, anxiety, and substance use disorder) during treatment periods compared with non-use periods in the same individuals. Randomized trials are needed to establish whether this association reflects a true therapeutic benefit.
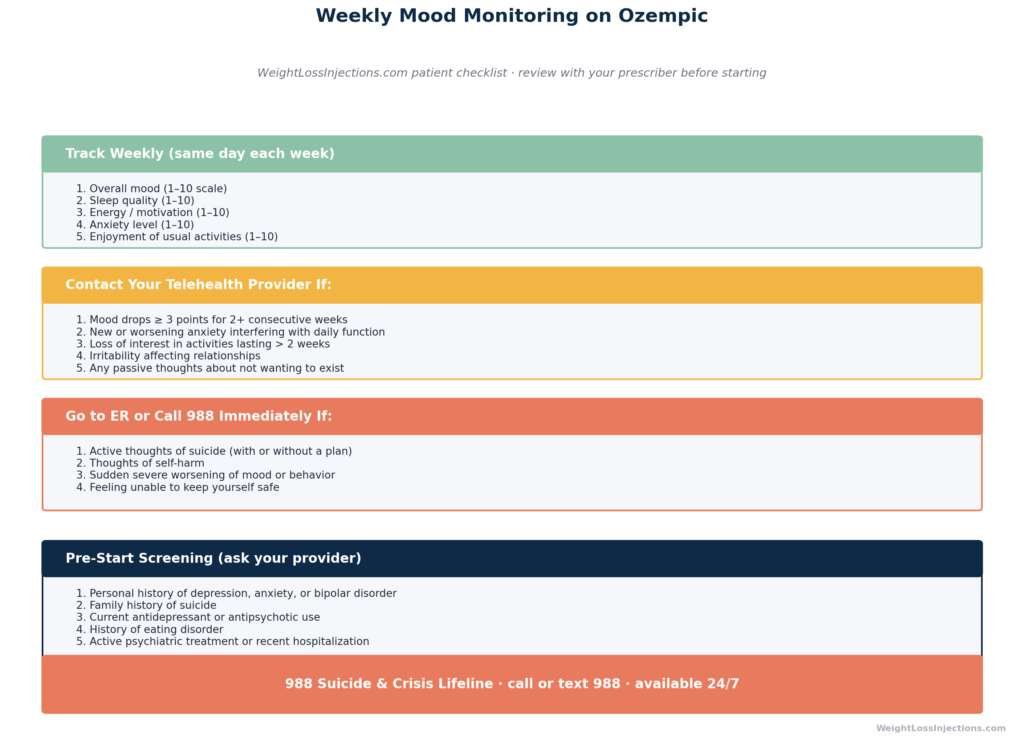
Mood Monitoring Checklist Infographic
Why Might Ozempic Affect Mood?
Understanding the biology here requires holding two possibilities simultaneously: GLP-1 receptor signaling in the brain may in some individuals blunt reward responsiveness broadly (potentially causing mood changes), while in others the same signaling pathways may reduce neuroinflammation and improve dopamine balance (potentially improving mood). The same pharmacology produces directionally opposite effects in different patient contexts.
GLP-1 Receptors in the Brain
GLP-1 receptors (GLP-1Rs) are widely distributed in the central nervous system, including in the hypothalamus, hippocampus, amygdala, dorsal raphe nucleus, and the mesolimbic dopamine circuit (Frontiers in Pharmacology, 2020). These regions regulate appetite, reward, emotional processing, memory, and stress response. GLP-1 signaling modulates dopamine activity in the VTA, the brain’s principal reward center, primarily by reducing dopaminergic output through inhibitory GABA interneurons, which reduces food- and substance-related craving (PMC Neuroscience Applied, 2025).
This craving-reduction is clinically useful. It becomes a theoretical problem when the same dopaminergic dampening extends beyond food-related reward, reducing hedonic response to social interaction, music, exercise, and other pleasurable activities, the neurobiological substrate of anhedonia. Whether this broader blunting occurs with any clinical frequency in humans is not established by controlled trial data; case series and pharmacovigilance reports suggest it may occur in a minority of susceptible individuals.
The case reports in Frontiers in Psychiatry (2023) proposed a specific mechanism: semaglutide increases dopamine transporter expression on neuronal surfaces in the lateral septum and striatum, which reduces available synaptic dopamine and may produce anhedonia-like states. This is a plausible but unconfirmed hypothesis derived from animal data and two human cases.
The Weight Loss Confound
Rapid weight loss, especially at a rate of 1–2 kg per week, can itself disrupt mood through several mechanisms: hormonal shifts (estrogen and testosterone decline as adipose tissue decreases), HPA axis activation from caloric restriction, and disruption of eating behaviors that may have functioned as emotional regulation strategies. Calm summarized the expert view: “Ozempic personality” symptoms may reflect the psychological difficulty of eating less, losing food as a source of comfort, and metabolic adjustment, not a direct neuropharmacological effect of semaglutide itself.
Baseline Psychiatric Comorbidity
Obesity and type 2 diabetes, the two primary indications for semaglutide, are each independently associated with substantially elevated rates of depression and anxiety. Patients prescribed Ozempic therefore start from a higher psychiatric risk baseline than the general population. This baseline elevation is the core confound that even well-designed observational studies struggle to fully eliminate, and it almost certainly contributes to the elevated psychiatric event rates observed in pharmacovigilance databases and in the Kornelius 2024 cohort study.
Patients at Higher Risk
Certain patient profiles warrant heightened vigilance before and during Ozempic therapy:
- History of major depressive disorder or recurrent depression — the Frontiers in Psychiatry case series included a patient with a history of three depressive episodes who experienced a severe relapse approximately one month after semaglutide initiation; symptoms improved after discontinuation and medication adjustment.
- Current antidepressant use — the WHO pharmacovigilance study found the suicidal ideation reporting signal was amplified (OR ~4.45) in patients taking antidepressants concurrently with semaglutide (The Pharmaceutical Journal, 2024), consistent with a hypothesis of additive vulnerability rather than semaglutide-specific causation.
- History of anxiety disorders, eating disorders, or substance use disorders — conditions sharing neurobiological overlap with the dopaminergic reward pathways modulated by GLP-1 receptor activation.
- Family history of suicide or bipolar disorder — where baseline genetic risk amplifies the significance of any new psychiatric stressor.
- Patients in the Kornelius et al. obesity cohort characteristics — namely those with obesity and without strong psychiatric support systems — appear to have the highest observed psychiatric event rates in the available observational literature, reinforcing the need for pre-treatment screening in this population.
None of these characteristics constitute a contraindication to Ozempic therapy — the drug’s glycemic and cardiovascular benefits are substantial and may outweigh psychiatric risks for most patients. They do constitute reasons to establish a psychiatric baseline, implement systematic mood monitoring, and maintain closer follow-up.
What Patients Should Do: A Practical Protocol
Before Starting Ozempic
Discuss the following with your prescribing provider or telehealth clinician at WeightLossInjections.com — [service detail]:
- Mental health history screening: Disclose any personal or family history of depression, anxiety, bipolar disorder, eating disorders, suicidal ideation, or suicide attempts. This enables your provider to set an appropriate monitoring intensity before prescribing.
- Current medications: Antidepressants, antipsychotics, and mood stabilizers interact with the risk profile discussed above and should be reviewed.
- Establish a baseline mood score: Use a validated brief instrument such as the PHQ-9 (depression) or GAD-7 (anxiety) at baseline so that subsequent changes are measurable rather than estimated.
A WeightLossInjections.com telehealth visit begins with a comprehensive intake that covers psychiatric history as part of the standard prescribing protocol — [$X/month] for bundled telehealth and medication coordination ([service detail]).
Weekly Mood Logging
After starting Ozempic, log mood weekly using a simple 1–10 scale across five domains: overall mood, sleep quality, energy/motivation, anxiety, and enjoyment of usual activities. A drop of 3 or more points from your personal baseline on two consecutive weekly assessments warrants a provider contact — not a panic response, but a clinical conversation. Many mood fluctuations on Ozempic are transient and correlate with the dose-escalation window, similar to the GI side effect pattern; they resolve once the body adjusts.
When to Contact Your Telehealth Provider
- Mood score decline of ≥3 points from baseline on two or more consecutive weekly assessments
- New onset of persistent anxiety, panic episodes, or irritability that interferes with daily function
- Loss of interest in previously enjoyed activities lasting more than two weeks
- Any passive thoughts about death, not wanting to exist, or feeling like a burden to others
- Uncertainty about whether your mood change is significant — err on the side of contact
When to Seek Urgent Help
Active suicidal ideation, meaning you have thoughts of killing yourself, with or without a specific plan, is a psychiatric emergency. The following symptoms require immediate action:
- Thoughts of suicide or self-harm, with or without intent to act
- Formulating or researching a plan for suicide
- Giving away possessions or saying goodbye in unusual ways
- Sudden calmness after a period of severe depression (can signal a decision to act)
- Any inability to keep yourself safe
Do not adjust your Ozempic dose, do not wait for a telehealth appointment, and do not call your prescribing provider’s routine line. Go to your nearest emergency department or call/text 988 (the Suicide and Crisis Lifeline, available 24/7).
If you have a firearm or other lethal means at home and are having suicidal thoughts, ask a trusted person to remove or secure them before your condition escalates. This single step — means restriction — is among the strongest evidence-based suicide prevention interventions available (FDA Drug Safety Communication, January 2026).
Our take at WeightLossInjections.com: The evidence on Ozempic and mental health is genuinely complex — and any content that presents it as simply dangerous or simply safe is doing patients a disservice. The FDA’s January 2026 conclusion, based on the largest analysis to date (91 trials, 107,910 patients), is reassuring: no causal link to depression, anxiety, or suicidal ideation has been established. At the same time, the Kornelius 2024 observational findings in obesity patients are a real signal that cannot be dismissed, even if confounding almost certainly explains part of it. Our clinical approach at WeightLossInjections.com is to treat psychiatric screening as a non-optional part of the Ozempic pre-start consultation — not because we believe the drug causes psychiatric harm in most patients, but because the patients who are most likely to benefit from Ozempic (those with obesity, T2DM, and metabolic disease) are the same patients who carry the highest baseline psychiatric risk. Good monitoring costs almost nothing; missed depression can cost everything.
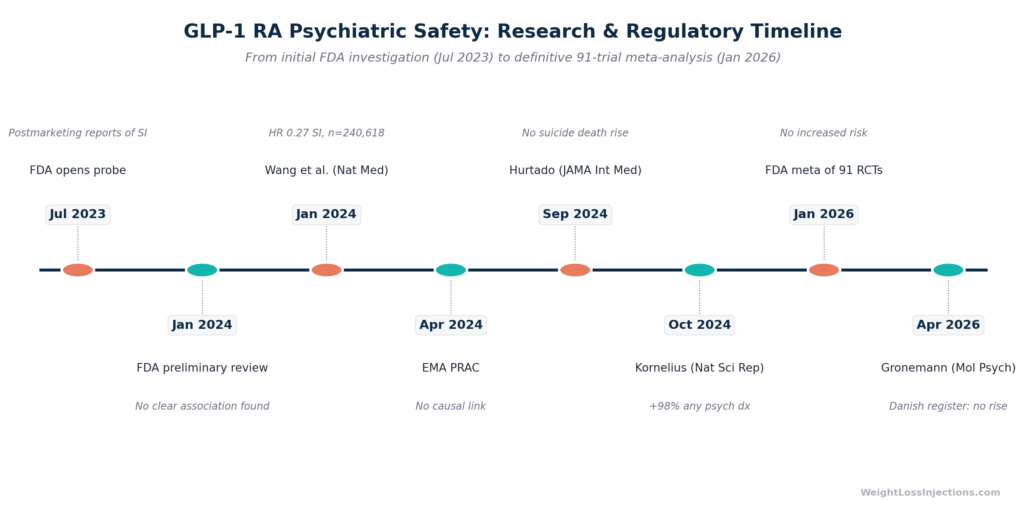
Inline, Timeline of Regulatory and Research Events on GLP-1 Psychiatric Safety
Frequently Asked Questions
Does Ozempic cause depression?
Based on the available evidence, Ozempic has not been established as a cause of depression. The current Ozempic prescribing information (2025) contains no depression warning. The FDA’s January 2026 comprehensive review — which included a meta-analysis of 91 clinical trials with 107,910 participants, found no increased risk of depression. Individual cases of depression emerging during semaglutide treatment have been reported, and a large 2024 observational study found higher depression rates in an obesity cohort using GLP-1 RAs; however, patients with obesity have substantially higher baseline depression risk, making it difficult to attribute those rates to the drug. If you develop symptoms of depression after starting Ozempic, contact your provider regardless of cause, the medication can be adjusted or discontinued.
Is anxiety a side effect of Ozempic?
Anxiety is not listed as a side effect in the Ozempic prescribing information (2025), and the FDA’s January 2026 review found no increased risk of anxiety with GLP-1 RA use. However, anxiety symptoms have been reported in pharmacovigilance databases and are part of the informal “Ozempic personality” cluster described by some patients. Proposed mechanisms include GLP-1 receptor effects on the amygdala, which regulates fear and anxiety responses, and the physiological stress of rapid weight loss on the HPA axis. Most reports of anxiety in the available case data are mild to moderate and transient. If anxiety is new, worsening, or impairing daily function, it warrants a provider conversation — dose adjustment, dietary support, or referral to a mental health professional may help.
Ozempic and suicidal thoughts: what is the real risk?
The weight of current evidence, including the FDA’s January 2026 meta-analysis of 107,910 patients, the Nature Medicine 2024 EHR cohort of more than 1.8 million patients, and a 2026 nationwide Danish register study, does not support a causal link between semaglutide and suicidal ideation. Multiple large studies have found lower suicidal ideation rates in semaglutide users compared with alternative medications. One large 2024 observational study in obesity patients found elevated suicidal behavior rates; however, that population carries a substantially elevated baseline psychiatric risk. Suicidal ideation has been reported in pharmacovigilance databases (40 semaglutide cases in one EudraVigilance analysis), but these counts are very low relative to the millions using the drug. If you experience thoughts of suicide while taking Ozempic, contact 988 (Suicide and Crisis Lifeline) or go to an emergency department immediately, do not delay because you attribute the thought to the medication.
What is “Ozempic personality”?
“Ozempic personality” is a colloquial, non-clinical term that emerged in media coverage in 2023–2024 to describe reported changes in mood and demeanor in some GLP-1 medication users. The most commonly described features are increased irritability, emotional flatness or numbness (anhedonia), lower energy or motivation, and reduced interest in previously enjoyable activities. Experts including those cited by Healthline dispute the term and emphasize that no controlled trial evidence supports a direct pharmacological cause. The proposed biological explanation, that GLP-1 receptor activation dampens dopaminergic reward signaling broadly, not just food-related reward, is plausible but unproven in humans. An equally valid explanation is that the significant behavioral change of eating less and losing weight rapidly is itself psychologically challenging and may account for many reported mood changes. If you notice a meaningful personality change or emotional shift that concerns you or others, discuss it with your provider rather than assuming it is the medication.
Should I stop Ozempic if I notice mood changes?
Do not stop Ozempic without speaking to your provider first. The FDA recommends patients not discontinue GLP-1 RA therapy without medical guidance, as stopping abruptly may worsen the underlying conditions being treated (type 2 diabetes, cardiovascular risk). Minor mood fluctuations, mild irritability or transient low energy, during dose escalation are common and often resolve within two to four weeks without any change to treatment. If symptoms are more severe, are worsening over time, or include any thoughts of self-harm, contact your provider promptly. In those cases, the provider may recommend a dose reduction, a treatment pause, referral to a mental health professional, or discontinuation, based on a risk-benefit evaluation for your individual circumstances.