![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/04/hero_ozempic_c5_lifestyle-1200x675.png)
STEP 1 Body Composition Changes: Fat Mass vs Lean Mass on Semaglutide
“Ozempic legs” is a social-media phrase, not a medical diagnosis. It describes the sagging skin, reduced muscle tone, and thinned appearance of the lower body that can follow rapid semaglutide-driven weight loss. The underlying cause is a combination of fat loss, lean-mass erosion, and skin laxity, all predictable consequences of fast weight loss. They are not inevitable. Evidence-based countermeasures, adequate protein, consistent resistance training, and gradual titration, can substantially reduce the effect. This article covers the trial data, the mechanisms, and a concrete prevention protocol.
Editorial note: This article is for educational purposes only. It is not a substitute for individualized medical advice. If you have concerns about body composition, muscle loss, or skin changes while on any GLP-1 medication, discuss them with your prescriber.
What Are “Ozempic Legs”?
“Ozempic legs” is an informal, patient-coined term that surfaced on social media as before-and-after photos of people using semaglutide (Ozempic, Wegovy) went viral. It describes a cluster of visible lower-body changes, primarily affecting the thighs and calves, that can appear after rapid, significant weight loss on semaglutide. The changes include:
- Sagging or “deflated” thigh skin — excess skin that previously stretched over adipose tissue has lost its underlying support
- Reduced muscle tone and definition — legs look thinner and softer, not lean and athletic
- More visible cellulite — as fat pads shrink, the skin surface can become uneven
- An overall frail or “wasted” appearance, especially in older adults losing weight quickly
None of these is a named adverse event in the FDA Ozempic Prescribing Information (2025). They are cosmetic and functional consequences of how rapid weight loss affects body composition and skin integrity, not a direct drug toxicity. That distinction matters, and we return to it in the “Ozempic Legs vs. Real Side Effects” section below.
“Ozempic legs” can follow weight loss from Wegovy, off-label Ozempic, or any other GLP-1 medication that produces substantial and rapid caloric restriction. The term has stuck partly because of the speed and magnitude of loss semaglutide enables, up to 14.9% of body weight at 68 weeks in the STEP 1 trial (NEJM, 2021). Losing that much weight in roughly 16 months is faster than most prior non-surgical methods, and faster loss generally means less time for skin and muscle adaptation.
Causes of Ozempic Legs
Three overlapping mechanisms drive the appearance of “Ozempic legs.” Understanding each one is necessary because the prevention strategies for each differ.
Fat Loss in the Legs
Semaglutide works by activating GLP-1 receptors in the hypothalamus and gut, suppressing appetite and slowing gastric emptying. The result is a sustained caloric deficit that leads to total body fat reduction. Fat loss is not evenly distributed: the lower body, particularly the thighs, inner knees, and gluteal area, holds a large proportion of subcutaneous adipose tissue, especially in women. As this fat diminishes, the structural “padding” under the skin disappears.
This is essentially the same mechanism behind loose skin after bariatric surgery, just occurring over a shorter period than most surgical patients experience historically. The clinical consequence is what aesthetic clinicians sometimes call a “deflation” effect, the skin surface remains while the volume beneath it contracts. As Medical News Today describes, fat loss exposes underlying structures that were previously obscured, including cellulite and skin creasing.
Muscle (Lean Mass) Loss
This is the mechanism most clinically relevant to the “Ozempic legs” appearance, and the one supported by the strongest primary data.
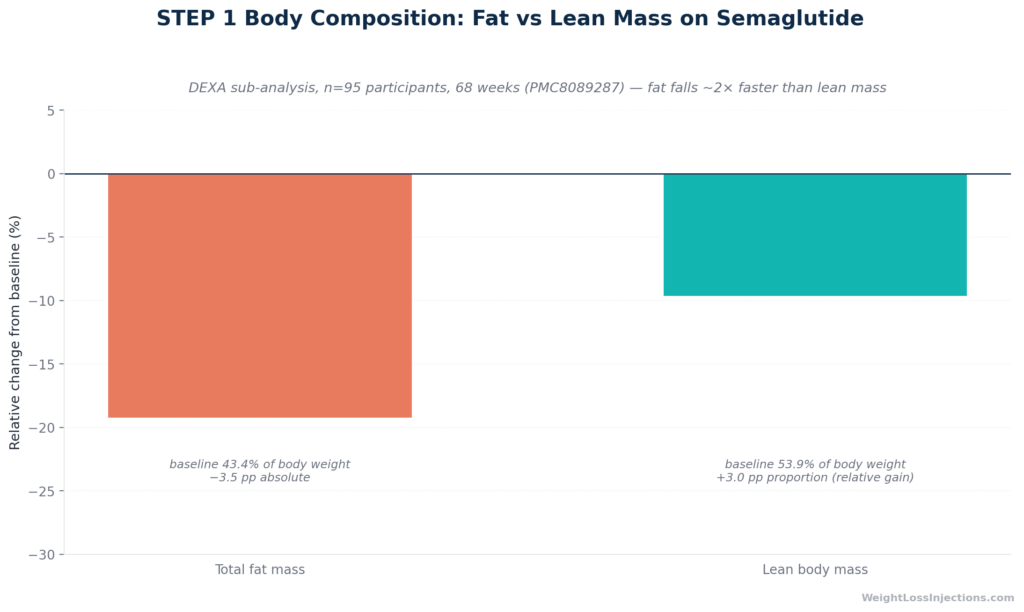
The landmark evidence comes from a body composition sub-study of the STEP 1 trial, published in 2021 and indexed as PMC8089287. Using dual-energy X-ray absorptiometry (DEXA) in 95 semaglutide-treated and 45 placebo-treated participants over 68 weeks, the sub-analysis found:
| Measure | Semaglutide (week 68 vs. baseline) | Placebo |
|---|---|---|
| Total body weight | −15.0% | −3.6% |
| Total fat mass | −19.3% | minimal change |
| Regional visceral fat mass | −27.4% | minimal change |
| Total lean body mass | −9.7% | minimal change |
| Lean mass proportion of total body weight | +3.0 percentage points (improved ratio) | no change |
The headline finding is nuanced: in absolute terms, lean body mass fell by 9.7%. In relative terms, because fat was lost faster than lean mass, the proportion of body mass that is lean tissue actually improved by 3.0 percentage points. The lean:fat ratio increased by 0.23 in the semaglutide group, and by 0.41 in participants who lost 15% or more of body weight.
This sounds reassuring, but the absolute lean mass loss is not trivial. A person starting at 100 kg with a 54 kg lean body mass who loses 15 kg total on semaglutide can expect to lose roughly 1.4–1.5 kg of that as lean mass — including skeletal muscle. A 2024 systematic review in Expert Opinion on Pharmacotherapy reviewed six clinical trials (1,541 participants) and found lean mass loss as a proportion of total weight lost ranged from approximately 0% to 40%, depending on the trial and patient population.
Importantly, semaglutide does not pharmacologically target skeletal muscle. As Fella Health notes, GLP-1 receptors have limited expression in skeletal muscle tissue. The lean mass loss occurs because the caloric deficit created by appetite suppression forces the body to catabolize both fat and muscle for energy, particularly in the absence of resistance training or adequate protein intake. The medication creates the conditions; lifestyle factors determine the outcome.
The clinical implication is significant. When legs lose both subcutaneous fat and underlying muscle, the visual result is precisely what social media has labeled “Ozempic legs”, thin, soft-looking, low-tone limbs. The SAGE Open Medicine case series (2025) showed that with structured resistance training (3–5 days/week) and intentional protein intake, two of three patients actually increased lean soft tissue while losing 13–33% of total body weight, demonstrating that substantial lean mass preservation is achievable.
Skin Laxity
Rapid weight loss, regardless of method, stresses collagen and elastin, the structural proteins that give skin its firmness and rebound capacity. A histological study published in ePlasty (2015) analyzed skin biopsies in patients following massive weight loss and found significantly lower collagen density and thinner collagen fibers in the reticular dermis compared to normal-weight controls, with complete or near-complete loss of elastic fiber network in some samples.
The practical consequence: skin that has been stretched by adiposity for years does not retract proportionally when the underlying volume is rapidly removed. As Healthline describes, when skin remains significantly stretched for prolonged periods, collagen and elastin fibers become damaged and lose their retraction ability. Several factors worsen skin laxity after GLP-1 weight loss:
- Age over 40 — natural decline in collagen production (~1% per year after the mid-30s) reduces rebound capacity (SLMD Skincare / Sandra Lee, MD)
- Greater magnitude of weight loss — more weight lost means more stretched skin to retract
- Faster rate of loss — less time for progressive skin remodeling
- Sun damage and smoking history — both impair existing collagen and elastin quality
- Prior obesity duration — longer periods of skin stretching predict more laxity
Skin laxity is the hardest component of “Ozempic legs” to prevent or reverse without professional intervention, but topical hydration, nutrition, and gradual loss rates all influence outcomes at the margin.
Prevention: Keep Legs Toned on Ozempic
Prevention is far more effective than treatment. The window for intervention is during active weight loss, not after the fact. The four strategies below address each of the three causes above and are supported by clinical evidence.
Protein Intake: Hit 1.0–1.6 g/kg Ideal Body Weight Daily
Protein is the primary nutritional lever for lean mass preservation during a caloric deficit. Amino acids from dietary protein signal muscle protein synthesis and provide substrate for muscle repair. On GLP-1 therapy, appetite suppression often reduces total food intake to the point where protein targets become difficult to meet passively, making deliberate tracking essential.
The evidence-based target for GLP-1 users is 1.0–1.6 g of protein per kg of ideal body weight daily, with some protocols going higher for active individuals. For reference:
| Body weight | Target protein range (1.0–1.6 g/kg IBW) |
|---|---|
| 140 lb (64 kg) | 64–102 g/day |
| 180 lb (82 kg) | 82–131 g/day |
| 220 lb (100 kg) | 100–160 g/day |
| 260 lb (118 kg) | 118–189 g/day |
IBW = ideal body weight; use 22.5 × height in meters² as a practical estimate.
These ranges align with recommendations from Medical News Today (experts interviewed, 2025), David Protein’s clinical review (2026), and the Ubie Doctor’s Note summary (2026). The Mass General Advances in Motion review (2025) adds that combining high-protein diet with exercise produces better lean mass preservation than either intervention alone.
Practical per-meal targets: Distribute protein across three to four meals, aiming for 25–40 g per meal. Consolidated protein is utilized more efficiently for muscle protein synthesis than large infrequent loads. High-quality sources with complete amino acid profiles include:
- Chicken breast (31 g per 100 g cooked)
- Greek yogurt (17 g per 170 g serving)
- Cottage cheese (14 g per 113 g / half cup)
- Eggs (6 g per egg; 18 g for three eggs)
- White fish — cod, tilapia (20–22 g per 85 g serving)
- Tofu, firm (10 g per 85 g serving)
- Whey or plant-based protein shake (20–30 g per scoop)
Because semaglutide reduces appetite globally, many patients on GLP-1 therapy spontaneously reduce protein below maintenance needs. Protein shakes are a practical bridge when solid food feels unappealing, particularly in the first weeks at a new dose.
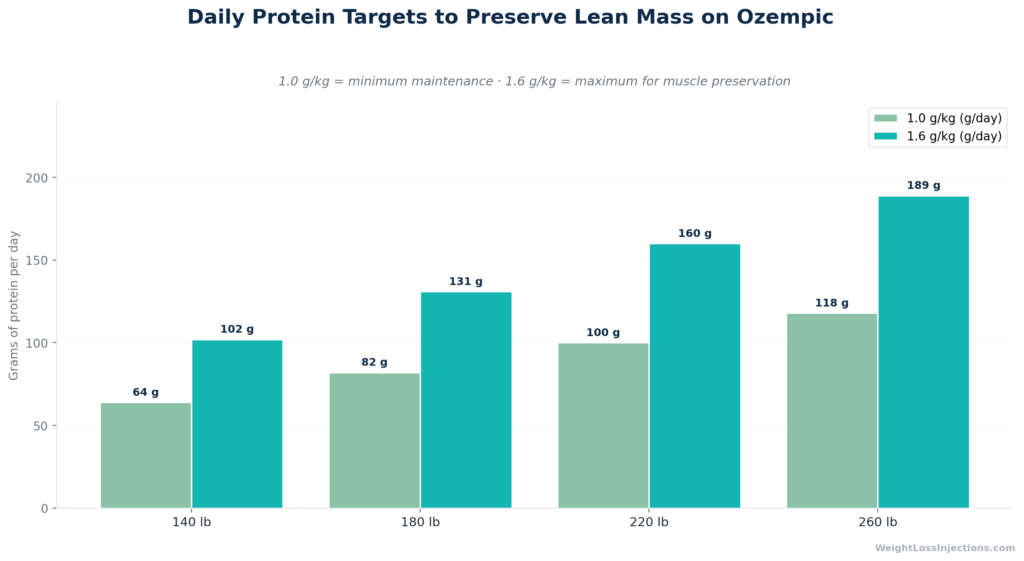
Protein Targets for GLP-1 Users by Body Weight
Strength Training: 2–3 Sessions per Week, Legs-Focused
Resistance training is the most important behavioral intervention for lean mass preservation during GLP-1-driven weight loss. It provides a mechanical signal, myofibrillar tension, that tells the body to retain skeletal muscle tissue even in a caloric deficit. Cardiovascular exercise does not provide this signal, and excessive cardio during a deficit can actively worsen lean mass loss by increasing total energy demand without triggering preservation pathways.
The American College of Sports Medicine recommends resistance training targeting all major muscle groups at least twice weekly for adults; the specific context of GLP-1 therapy makes this recommendation especially important. Mass General’s endocrinology team (2025) reports that patients who engage in regular exercise at treatment initiation have the best chances of preserving lean body mass.
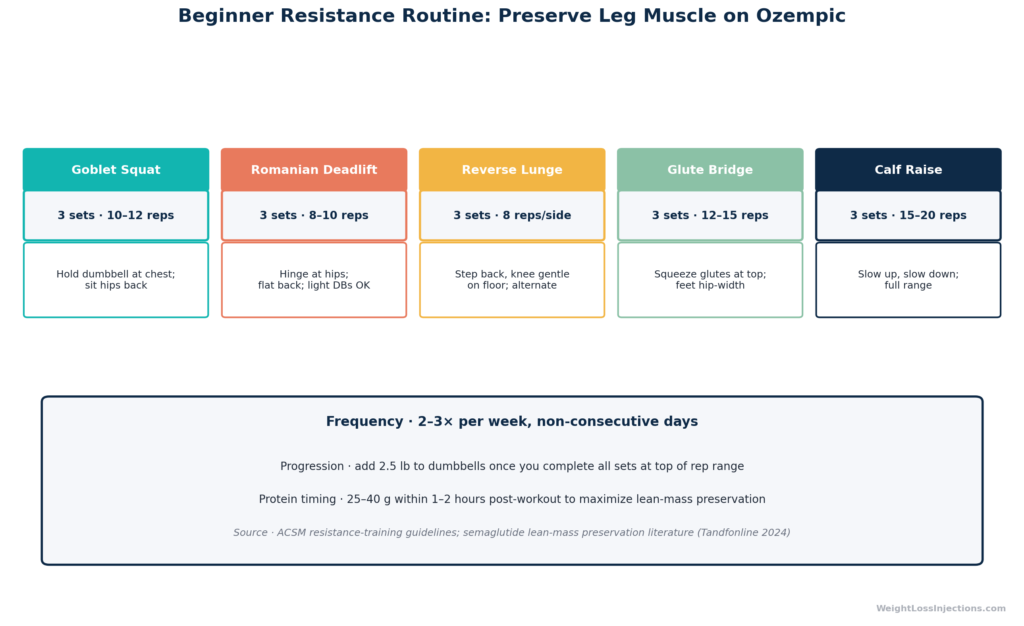
For “Ozempic legs” specifically, a lower-body emphasis two to three times per week is appropriate. The following compound movements recruit the quadriceps, hamstrings, gluteal muscles, and calves simultaneously, maximizing stimulus per unit of workout time:
Beginner protocol (weeks 1–6):
| Exercise | Sets × Reps | Notes |
|---|---|---|
| Goblet squat | 3 × 10–12 | Heels shoulder-width; dumbbell or kettlebell at chest |
| Romanian deadlift | 3 × 10–12 | Hip hinge; dumbbells; feel hamstring stretch at bottom |
| Reverse lunge | 3 × 10–12 per leg | Controlled descent; keep front knee over ankle |
| Glute bridge | 3 × 15 | Pause 1 second at top; can add dumbbell on hips |
| Calf raise | 3 × 15–20 | Use step edge for full range of motion |
Rest 60–90 seconds between sets. Total session time: 30–40 minutes. As a general note, moderate-to-heavy loads in the 6–12 rep range provide a stronger muscle-preservation stimulus than very light weights in the 20+ rep range, though any consistent resistance training is beneficial for GLP-1 users who are currently sedentary.
Progression (weeks 7+): Increase resistance or add one set when three sets feel manageable. The Maik Wiedenbach analysis (2026) estimates that GLP-1 users combining strength training with adequate protein can reduce lean mass loss from 25–40% of total weight lost down to approximately 10–15%. The SAGE Open Medicine case series (2025) documented two patients who actually gained lean soft tissue despite losing 13–33% total body weight through structured resistance training 3–5 days/week.
Allow 48 hours between sessions targeting the same muscle groups. Walking daily (7,500–10,000 steps) complements the strength work without adding excessive catabolic demand.
Gradual Titration: Target 1–2 lb per Week Loss
Rate of weight loss directly affects the ratio of fat to lean mass lost and the degree of skin laxity that develops. As Medical News Today notes, rapid weight loss increases muscle loss and reduces the time available for skin adaptation, both of which worsen the “Ozempic legs” appearance.
A loss rate of 1–2 lb per week is the generally accepted target for sustainable, composition-preserving weight loss. On semaglutide, titration schedule directly influences loss rate: patients who rush escalation or jump to higher doses without need often achieve faster loss but at the cost of lean mass and skin quality. The FDA Ozempic Prescribing Information (2025) requires a minimum of four weeks at each dose step before escalation, a schedule that coincidentally aligns with body-composition protection goals.
Clinically, a prescriber can hold a patient at a lower maintenance dose if weight loss is already occurring at an acceptable rate, rather than escalating on a fixed calendar. This is a legitimate clinical decision that your provider can make based on your individual response. If you are losing weight faster than 2 lb/week and experiencing body composition concerns, ask your prescriber whether slowing titration is appropriate.
Hydration and Skin Support
Hydration directly affects skin turgor and surface appearance. Dehydrated skin accentuates creasing, cellulite visibility, and the “deflated” look. Target at least 2 liters (8+ glasses) of water daily, or more if you are exercising or in a hot environment.
For topical support, moisturizers containing hyaluronic acid, ceramides, or peptides can improve skin barrier function and surface appearance. Hyaluronic acid draws water into the skin. Ceramides reinforce the lipid barrier that retains it. These products cannot reverse established skin laxity, but they reduce the cosmetic burden while underlying conditions improve. Body brushing and massage may improve circulation but have no established evidence for reversing skin laxity.
Collagen supplements (hydrolyzed collagen, 5–10 g/day) have shown modest evidence for improving skin hydration and elasticity in controlled trials, as Healthline summarizes. The effect is not specific to post-GLP-1 skin, but the intervention has a good safety profile and addresses a plausible mechanism. Vitamin C supports collagen synthesis and is best obtained through dietary sources (citrus, bell peppers, broccoli) rather than high-dose supplementation.
Our Top 3 · August 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
Treatments If You Already Have Ozempic Legs
If body composition changes are already established, the same interventions described above remain the first-line approach, they work in reverse as well as in prevention.
Rebuild lean mass through resistance training and protein. Muscle can be rebuilt post-weight loss; the process is slower than preservation but clinically achievable. The combination of protein 1.2–1.6 g/kg daily and consistent resistance training is the foundation. The Mass General review (2025) confirms that diet plus exercise outperforms either alone for body composition outcomes.
Non-surgical aesthetic options: For skin laxity and cellulite visibility, radiofrequency (RF) and ultrasound-based devices (performed by a board-certified dermatologist or plastic surgeon) have evidence for modest skin tightening. These are cosmetic procedures, not covered by insurance, and their results in the specific context of GLP-1-related skin laxity have not been evaluated in controlled trials. Consult a dermatologist for individualized assessment. Manage expectations: non-surgical devices produce gradual, modest improvement, not the results of surgical body contouring.
Surgical options — including thigh lift and body contouring procedures — exist for patients with severe, functionally limiting excess skin. These are appropriate only after weight has been stable for 12–18 months and are beyond the scope of telehealth management. A plastic surgeon with experience in post-weight-loss body contouring should be consulted.

Prevention and Treatment Flowchart for Ozempic Legs
Prevention and Treatment Flowchart for Ozempic Legs
Ozempic Legs vs. Real Medical Side Effects
“Ozempic legs” is a cosmetic and functional concern, not a medical adverse event. It is important to distinguish it clearly from symptoms that require clinical evaluation.
What “Ozempic Legs” Is Not
Leg pain, cramps, or weakness are not components of “Ozempic legs” and should not be dismissed as a cosmetic issue. Muscle cramps during semaglutide treatment have a distinct and separate mechanism. Per the FDA Ozempic Prescribing Information (2025), semaglutide’s GI side effects, nausea, vomiting, diarrhea, can cause dehydration and volume depletion, which the FDA warns can lead to acute kidney injury if severe. The FDA label specifically advises monitoring renal function in patients with adverse reactions that could cause volume depletion.
Leg cramps on semaglutide are not listed as a formal adverse effect in the FDA prescribing information, but as Bolt Pharmacy (2025) explains, indirect mechanisms are plausible: GI-driven dehydration and electrolyte depletion (sodium, potassium, magnesium, calcium) are well-recognized triggers for muscle cramping. The Fella Health guide (2025) notes that reduced carbohydrate intake on GLP-1 therapy also increases renal sodium excretion, further affecting fluid and electrolyte balance.
A Practical Distinction
| Symptom | Category | Action |
|---|---|---|
| Sagging thigh skin | Cosmetic / body composition | Protein + resistance training; dermatologist if persistent |
| Reduced muscle definition in legs | Body composition | Resistance training + protein protocol |
| Leg muscle cramps | Possible electrolyte/dehydration issue | Hydrate; review electrolytes (K, Mg, Na); contact prescriber if recurrent |
| Persistent leg pain or weakness | Possible medical AE | Contact prescriber promptly |
| Myalgia with extreme fatigue, dark urine | Possible serious AE (rare rhabdomyolysis reported in case literature) | Seek immediate medical evaluation |
| Signs of dehydration (dizziness, dark urine, inability to keep fluids down) | Potential serious AE per FDA label | Contact prescriber or seek urgent care |
A case report in Cureus (2023) described rhabdomyolysis associated with semaglutide in one patient, an association not previously documented in the literature. This is not an established class effect, but it underscores that unexplained muscle weakness or severe myalgia on semaglutide warrants evaluation, not reassurance.
The cosmetic changes of “Ozempic legs” do not require emergency action. The medical symptoms above do.
WeightLossInjections.com: Monitoring Body Composition on GLP-1 Therapy
Our take at WeightLossInjections.com: “Ozempic legs” is preventable in most cases, but prevention requires proactive clinical management, not just a prescription and a monthly refill. A prescriber who is actively monitoring your titration pace, checking in on protein intake and exercise habits, and willing to hold a dose to protect body composition is meaningfully different from one who simply escalates on a fixed schedule. Body composition outcomes on semaglutide are not just about how much weight you lose, they’re about what you lose.
At WeightLossInjections.com, our telehealth [service detail] program includes structured onboarding that covers protein targets, resistance training recommendations, and titration monitoring for patients on GLP-1 medications. Our licensed providers review your history and goals before prescribing and remain available throughout your treatment. All-in monthly cost starts at [$X/month]. If you’re on semaglutide and not currently working with a provider who is monitoring your body composition plan, our GLP-1 intake quiz takes under 3 minutes, a licensed provider reviews your information within 24 hours.
One more note on the evidence: the STEP 1 DEXA sub-analysis showed that the lean:fat mass ratio improved in semaglutide-treated patients, which is the right headline. But that improvement was driven entirely by losing more fat than lean mass, not by preserving lean mass absolutely. The absolute lean mass loss is real, and in people already low in muscle reserve (older adults, sedentary individuals), it matters clinically. Do not let the ratio headline dismiss the intervention need.
Frequently Asked Questions
“Ozempic legs” results from three converging mechanisms: fat loss from the lower body (thighs, calves, gluteal area) that removes the structural padding under the skin; lean mass loss driven by the caloric deficit semaglutide creates; and skin laxity from collagen and elastin that cannot fully retract after rapid volume loss. The STEP 1 DEXA sub-analysis (PMC8089287) confirmed that absolute lean body mass falls 9.7% over 68 weeks on semaglutide 2.4 mg, and a 2024 systematic review found lean mass loss ranging from near 0% to 40% of total weight lost across trials. Semaglutide does not directly target muscle; the loss is a consequence of caloric restriction without countermeasures.
Yes, to a substantial degree. Resistance training 2–3 times per week, focused on compound lower-body movements like squats, lunges, and Romanian deadlifts, sends the mechanical signal that preserves skeletal muscle during a caloric deficit. The SAGE Open Medicine case series (2025) documented two patients who increased lean soft tissue while losing over 13% of body weight through structured resistance training 3–5 days/week. The Maik Wiedenbach analysis estimates that GLP-1 users combining strength training with adequate protein can reduce lean mass loss from 25–40% of total weight lost to approximately 10–15%. Exercise cannot prevent skin laxity entirely, but rebuilding muscle underneath adds volume that partially compensates for lost fat padding.
The recommended range for GLP-1 users is 1.0–1.6 g of protein per kg of ideal body weight daily, distributed across meals targeting 25–40 g per serving. For a 200 lb person, that translates to roughly 90–145 g/day. Medical News Today and David Protein’s clinical review align on this range. High-quality complete protein sources, chicken, Greek yogurt, eggs, fish, cottage cheese, and protein supplements when appetite is suppressed, should anchor each meal. Because semaglutide reduces total food intake, passive protein intake often falls short; deliberate tracking helps.
Not necessarily. The three components have different trajectories. Fat redistribution following stable weight can shift with continued exercise. Lean mass loss is reversible with consistent resistance training and adequate protein, muscle can be rebuilt, though the process takes months of sustained effort. Skin laxity is the most persistent component; mild to moderate laxity improves gradually with time, exercise, and hydration, but significant laxity after large weight losses may not fully resolve without aesthetic or surgical intervention. Non-surgical RF/ultrasound devices can provide modest improvement; surgical body contouring for severe cases should be discussed with a board-certified plastic surgeon after weight has been stable for 12–18 months.
“Ozempic legs” is a cosmetic term describing visible changes, loose skin, reduced tone, deflated appearance, that are not adverse events in the FDA Ozempic label. Leg muscle pain or cramps during semaglutide treatment are a separate concern, likely driven by indirect mechanisms: GI-related dehydration reduces volume and disrupts electrolyte balance (sodium, potassium, magnesium, calcium), all of which are required for normal muscle contraction. The FDA label warns specifically about dehydration risk from GI adverse reactions and acute kidney injury risk from volume depletion. If you experience recurring leg cramps, address hydration and electrolyte intake first and discuss with your prescriber. Severe, persistent muscle pain with weakness or very dark urine requires immediate medical evaluation, a rare case report described rhabdomyolysis associated with semaglutide (Cureus, 2023).
This article is for educational purposes only and is not a substitute for medical advice. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. If you are considering semaglutide or any GLP-1 medication, or are currently on one and experiencing body composition concerns, consult a licensed prescriber.
