Ozempic Before & After: Realistic Photos & Timelines
Medically reviewed by WeightLossInjections.com Staff•Updated July 23, 2026•15 min readMedically reviewed
⤢
Ozempic Weight Loss Timeline
On semaglutide at Ozempic doses (0.5–2 mg), trial and real-world data show roughly 5–6% body weight loss by month 3, 8–10% by month 6, and up to 10–14% by 12–17 months. “Ozempic face”, facial fat loss causing a gaunt appearance, is a real but manageable side effect tied to rapid weight loss, not a direct drug effect. Resistance training, adequate protein, and gradual titration all reduce the risk.
What Ozempic Does for Weight Loss
Ozempic (semaglutide injection) is FDA-approved for type 2 diabetes management, but its most visible effect is often significant weight reduction. The mechanism starts in the gut and brain: semaglutide is a GLP-1 receptor agonist that mimics the naturally occurring glucagon-like peptide-1 hormone. According to the Ozempic FDA prescribing information, semaglutide stimulates insulin secretion, suppresses glucagon, and, critically for weight, slows gastric emptying and signals satiety to hypothalamic centers in the brain.
The practical result is a meaningful reduction in appetite and caloric intake. Patients consistently report eating smaller portions without effort, losing cravings for high-calorie foods, and feeling full after less food. These effects are dose-dependent: higher doses produce stronger appetite suppression, which explains why the STEP trials using the higher 2.4 mg Wegovy dose tend to show larger percentage losses than real-world Ozempic users on 0.5–1 mg.
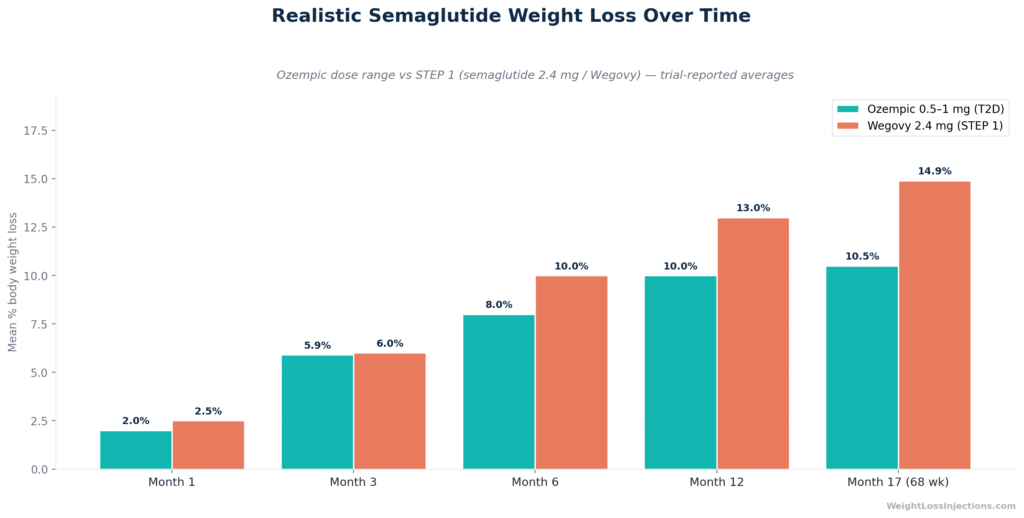
A landmark source for understanding outcomes at Ozempic’s dose range is the SUSTAIN-1 trial published in Diabetes Care, a 30-week phase 3 study in drug-naive type 2 diabetes patients. SUSTAIN-1 reported mean body weight losses of 4.5% on semaglutide 0.5 mg and 6.0% on semaglutide 1.0 mg, establishing the baseline for what the diabetes-approved dose range can do in a controlled clinical setting.
For patients using Ozempic off-label for weight loss (without type 2 diabetes), the largest real-world study comes from Ghusn et al. 2022 in JAMA Network Open, a Mayo Clinic dataset of 175 adults on subcutaneous semaglutide. That cohort lost a mean of 5.9% body weight at 3 months and 10.9% at 6 months, closely mirroring the trial data and providing a realistic anchor for non-diabetic patients at Ozempic doses.
The STEP 1 trial, which tested semaglutide 2.4 mg (the Wegovy dose), is the ceiling study: published in the New England Journal of Medicine, it reported 14.9% mean body weight reduction at 68 weeks in adults with obesity or overweight with a comorbidity. That benchmark is frequently cited in before-and-after discussions, but it reflects a dose higher than standard Ozempic. At Ozempic’s 1 mg maintenance dose, expect somewhat lower results, closer to 6–10% depending on individual factors.
Ozempic Before & After: Clinical Trial Timelines
The most common complaint about before-and-after content online is that photos exist without context, no starting weight, no dose, no duration. Trial data fills that gap with actual numbers.
Month 1–3: Approximately 2–6% Loss (Appetite Drop, Subtle Visual Changes)
During the titration phase, most patients start at 0.25 mg weekly for the first four weeks, then step to 0.5 mg. This cautious ramp exists to limit gastrointestinal side effects: according to the Ozempic FDA label, nausea occurs in 15.8% of patients at 0.5 mg versus 6.1% on placebo.
At the 3-month mark, the Ghusn 2022 real-world analysis in JAMA Network Open recorded a mean loss of 5.9% body weight in non-diabetic patients. For a 220-pound person, that is approximately 13 pounds. Visually, most patients report that others notice something has changed but cannot pinpoint what. Waistbands are looser; faces look a little less full. Before-and-after photos taken at this stage show subtle changes rather than dramatic ones.
Fat loss at this stage tends to occur from the trunk first, which is consistent with how GLP-1-mediated caloric restriction works — the same pattern seen with any caloric deficit. Facial changes are typically minimal at the 2–6% loss range unless the patient had significant facial fat to begin with.
Month 4–6: Approximately 6–10% Loss (Visible Body Shaping)
By months 4–6, most patients have titrated to 1 mg weekly (or higher for Wegovy dosing). This is where before-and-after photos become compelling. The STEP 4 trial in JAMA provides the most granular mid-study data: at the 20-week mark of the 68-week trial, participants on continuous semaglutide 2.4 mg had lost approximately 10.6% of body weight. The waist circumference reduction was −9.7 cm from baseline, a concrete physical measurement that translates into one to two pants sizes for many people.
For Ozempic doses (0.5–1 mg), the Ghusn 2022 Mayo Clinic dataset clocked 10.9% mean loss at 6 months, suggesting real-world results at Ozempic doses can approach the trial results at comparable durations.
At this stage, before-and-after photos typically show visible changes in the face, neck, upper arms, and waist. This is also when some patients first notice early facial hollowing, the phenomenon the media has labeled “Ozempic face.”
Year 1 and Beyond: 10–15% Loss (Significant but Gradual)
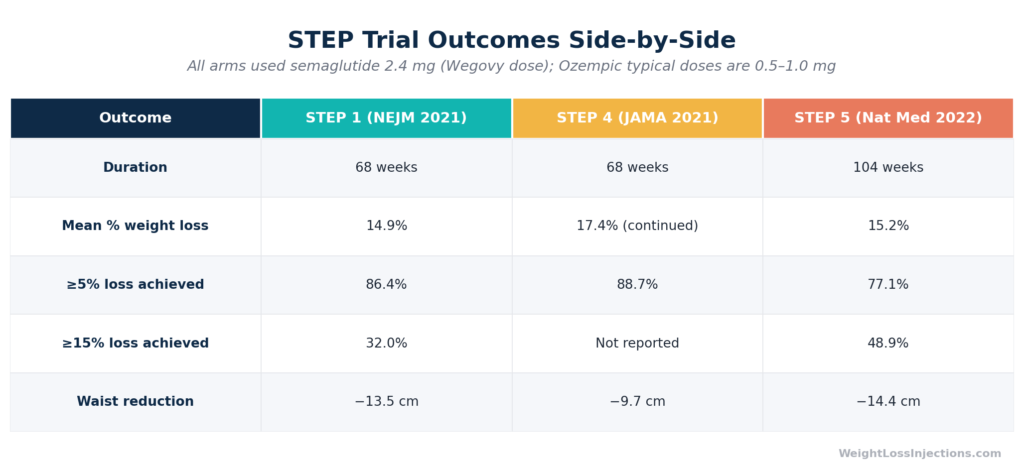
Long-term outcomes hinge on adherence and dose. The STEP 5 trial published in Nature Medicine followed patients on semaglutide 2.4 mg for 104 weeks (two years) and found a mean weight loss of 15.2%, demonstrating that results continue to accumulate past the 68-week STEP 1 endpoint. Crucially, STEP 5 found 77.1% of patients achieved at least 5% body weight loss and 48.9% achieved at least 15% loss, a meaningful spread showing the variability in individual response.
At Ozempic’s approved doses over 12 months, expect results in the 10–14% range based on the convergent evidence from SUSTAIN trials and real-world data. Before-and-after photos at this stage often show the most dramatic visible transformation: changes in face shape, neck, torso, and limbs that are unmistakable in side-by-side comparisons.
STEP Trial Outcomes Comparison
Real Ozempic Before & After: What Trial Data Actually Looks Like
You will find thousands of before-and-after photos on Reddit (r/Ozempic, r/GLP1), TikTok, and clinic websites. These serve a real motivational function, but they come with serious context problems: unknown starting weights, undisclosed doses, cherry-picked timelines, and no disclosure of concurrent interventions like diet programs or exercise. Dramatic celebrity transformations are even less informative, rapid visible weight changes in high-profile individuals are often attributed to Ozempic without confirmation, and are frequently achieved through additional measures including personal training, nutritionist support, and caloric restriction far beyond what the drug alone produces.
What trial data actually looks like in population terms: if you enrolled 100 people with obesity on semaglutide 2.4 mg for 68 weeks, the STEP 1 NEJM data shows you would expect roughly 86 of them to lose at least 5%, 69 to lose at least 10%, and 32 to lose at least 15%. Roughly 1 in 7 participants did not reach even 5% loss at the therapeutic dose. This spread is the honest before-and-after picture.
For Ozempic’s dose range in patients with type 2 diabetes, the SUSTAIN-6 trial published in NEJM, a cardiovascular outcomes study, documented mean weight losses of 3.6 kg (semaglutide 0.5 mg) and 4.9 kg (semaglutide 1 mg) over 104 weeks. In a population averaging roughly 92 kg at baseline, those are approximately 4–5% losses over two years, reflecting the diabetes-population dose range.
The honest answer to “what will I look like?” is: meaningfully different, but not at the pace or magnitude of the most viral transformation posts. The FDA Ozempic prescribing information does not include weight management as an indication for the drug, which is a reminder that even large average effects in trials contain a substantial range of individual outcomes.
Our Top 3 · August 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Ozempic Face: What It Is, What Causes It, and How to Manage It
“Ozempic face” is not an FDA-recognized medical term. It is a colloquial label, popularized by dermatologists and media in 2022–2023, for the gaunt, aged, or hollowed facial appearance that some patients experience after rapid significant weight loss — whether from semaglutide, other interventions, or any cause. The phenomenon is not unique to semaglutide: it occurs with any sustained rapid weight loss that depletes facial fat compartments.
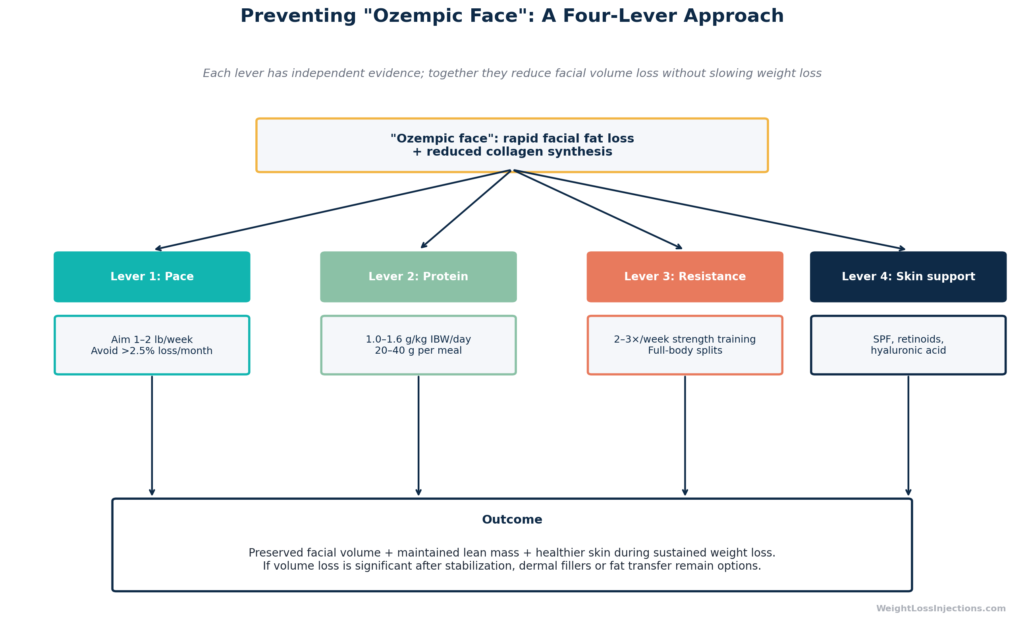
The mechanism is straightforward. The face contains multiple discrete fat pads — malar (cheek), buccal, temporal, and periorbital among them. These pads provide structural volume that gives a face its youthful contours. When total body fat decreases rapidly, the face loses volume disproportionately to other areas, because facial fat is not mechanically protected the way subcutaneous abdominal fat is. The result is hollowed cheeks, more prominent nasolabial folds, sunken temples, and a more angular jaw, features associated with aging.
The Role of Rate and Magnitude of Weight Loss
The critical variable is not the drug — it is the speed and total amount of weight lost. A 2023 review in the Journal of the American Academy of Dermatology noted that facial aging from weight loss is most pronounced when loss exceeds 10% of body weight over a short period, and that gradual loss over 12+ months is associated with less severe facial volume depletion than equivalent loss over 3–4 months. This has direct implications for dose titration strategy: patients who titrate slowly and stay at lower therapeutic doses (0.5–1 mg) rather than rapidly pushing to maximum doses may preserve facial volume better.
Prevention Strategy 1: Resistance Training
The most evidence-supported strategy for preserving facial and overall body composition during semaglutide-induced weight loss is resistance (strength) training. A 2022 analysis in Obesity published alongside STEP 3 data found that patients who combined semaglutide with intensive behavioral therapy including exercise preserved lean body mass more effectively than medication alone. Lean mass preservation, including the muscular support structures underlying facial tissue, is associated with a more favorable body composition outcome.
Practically: 2–3 sessions per week of resistance exercise (compound movements, progressive overload) is the standard recommendation from obesity medicine clinicians to minimize muscle and fat-free mass loss during GLP-1 therapy. AACE/ACE obesity clinical guidelines specifically recommend resistance training as an adjunct to pharmacotherapy for this reason.
Prevention Strategy 2: Adequate Dietary Protein
Protein intake is the nutritional lever most directly tied to lean mass preservation. The STEP 3 trial (JAMA, 2021) included an intensive dietary counseling component, and participants with the highest adherence to protein targets — approximately 1.2–1.5 g per kg of body weight daily — maintained lean mass better than those consuming lower protein amounts. For a 200-pound (91 kg) patient, that translates to roughly 110–135 grams of protein per day, achievable through a diet centered on lean meats, fish, eggs, dairy, and legumes.
Preserving lean body mass slows the visible appearance of facial aging from weight loss, because muscle and connective tissue underlying the face contributes to structural support even when fat pads decrease.
Prevention Strategy 3: Gradual Titration
The Ozempic dosing ladder — 0.25 mg × 4 weeks, then 0.5 mg, then 1 mg, then optionally 2 mg — exists to manage GI tolerability. But it has a secondary benefit: gradual loss. Per the Ozempic FDA label, the 0.25 mg starting dose is a non-therapeutic initiation dose, and most patients do not lose significant weight in the first 4–8 weeks. This slow start allows the body to adapt to caloric restriction gradually rather than experiencing an abrupt large deficit, which correlates with slower fat loss and better tissue adaptation.
Patients who resist pressure to rapidly escalate to maximum doses may preserve more facial volume — at the cost of a slower overall trajectory.
When Prevention Isn’t Enough: Aesthetic Options
For patients who do experience notable facial volume loss, several dermatologic interventions can restore volume:
Hyaluronic acid fillers (e.g., Juvederm Voluma, Restylane Lyft) are the most commonly used reversible option, adding volume to depleted malar and temporal fat compartments
Poly-L-lactic acid (Sculptra) stimulates collagen production over months, providing a more gradual volumizing effect
Fat transfer is a surgical option for patients seeking a more permanent solution
These are aesthetic choices, not medical necessities. The American Academy of Dermatology notes that weight regain — as commonly occurs when semaglutide is discontinued — typically restores facial volume to near pre-treatment levels, which is relevant for patients who are using Ozempic temporarily.
Factors That Affect Your Before-and-After Results
Trial averages describe populations, not individuals. Several factors modulate how much weight any given patient loses on semaglutide:
Starting BMI and weight. Patients with higher BMI tend to lose greater absolute weight but similar or slightly lower percentage weight loss compared to patients closer to the overweight/obesity threshold. The STEP 1 trial NEJM publication stratified by BMI quintile and found the broad middle of the BMI distribution (35–45) had the most consistent percentage outcomes.
Dose. This is the single largest modifiable variable. Semaglutide 2.4 mg (Wegovy) produces approximately 5–8 percentage points greater weight loss than semaglutide 0.5–1 mg (standard Ozempic doses), based on the STEP 1 versus SUSTAIN-1 comparison. Patients on standard Ozempic who tolerate it well may benefit from discussing the 2 mg dose, now FDA-approved for diabetes and increasingly used off-label, with their provider.
Diet quality. GLP-1 agonists suppress appetite but do not override diet composition. Patients who use reduced appetite as a cue to improve dietary quality (more protein, vegetables, whole foods; less ultra-processed food) tend to achieve better outcomes. A 2021 analysis in Metabolism found dietary adherence was a stronger predictor of weight loss on semaglutide than baseline BMI.
Exercise. As noted above, resistance training specifically preserves lean mass. Aerobic exercise adds incremental caloric expenditure but does not dramatically alter percentage weight loss in controlled trials, the appetite suppression from semaglutide is the dominant driver.
Adherence and continuity. The STEP 4 JAMA trial randomized patients who had already lost weight on semaglutide to either continue the drug or switch to placebo. The placebo group regained 6.9 percentage points of the lost weight within 48 weeks. This is the clearest clinical evidence that Ozempic’s results require ongoing use to maintain, and that before-and-after photos taken at treatment discontinuation do not represent where patients stay.
Ozempic Face Diagram
Getting Ozempic via Telehealth at WeightLossInjections.com
Ozempic requires a prescription, which means accessing it starts with a licensed provider evaluation. Telehealth has made that process significantly more efficient: at WeightLossInjections.com, patients complete a free online intake form that covers medical history, current medications, BMI, and weight-loss goals. A licensed provider reviews your information within 24 hours and, if appropriate, issues a prescription along with a personalized titration plan.
The bundled telehealth program at WeightLossInjections.com is [$X/month], which includes [service detail], making it a comprehensive option compared to sourcing medication and provider care separately.
For context on how this compares to out-of-pocket medication costs: Ozempic’s list price is $1,028/month, but patients using NovoCare Pharmacy can access it at $199/month for the first two fills (new patients, through June 30, 2026) and $349/month ongoing for 0.5–1 mg doses. A telehealth bundle that includes provider oversight and dose management alongside medication access offers a meaningful advantage for first-time GLP-1 users who need help navigating side effects and titration decisions.
Eligibility is assessed based on FDA-approved criteria from the Ozempic prescribing information: type 2 diabetes management is the labeled indication. Off-label use for weight loss requires provider discretion and patient history review. WeightLossInjections.com providers assess both pathways, start your free intake to find out which applies to your situation.
Our take at WeightLossInjections.com: The single most important decision in your Ozempic before-and-after journey is not which app to use or which photo to take, it is finding a provider who will actively manage your titration, respond to side effects promptly, and help you build the diet and exercise habits that turn drug-assisted appetite suppression into lasting change. Before-and-after photos from well-managed patients look different from those of patients who had no clinical support. That clinical layer is what WeightLossInjections.com is built around.
Frequently Asked Questions
How much weight can you lose on Ozempic in 3 months?
Based on the best available real-world data — the Ghusn 2022 Mayo Clinic cohort in JAMA Network Open — the mean body weight loss on semaglutide at 3 months is approximately 5.9%. For a 220-pound person, that is roughly 13 pounds. Individual results vary: some patients lose 3–4% at 3 months while still on the 0.5 mg titration dose; patients who escalate to 1 mg earlier and tolerate it well may approach 7–8%. The SUSTAIN-1 trial in Diabetes Care found 4.5–6.0% loss at 30 weeks in a type 2 diabetes population, providing a comparable anchor. Weight loss is rarely linear — most patients report the most rapid change in months 2–4, when appetite suppression is newly established and the deficit is largest relative to habitual intake.
What does Ozempic face look like before and after?
“Ozempic face” refers to facial hollowing, specifically loss of volume in the malar (cheek), buccal (jowl area), and temporal (temple) fat pads, creating a gaunt or aged appearance. Before treatment, faces appear fuller at the cheeks and temples; after significant weight loss, the same face may show more prominent cheekbones, deeper nasolabial folds, and a more angular jaw. The effect is most pronounced when weight loss is rapid — typically 15% or more of total body weight over less than 12 months. Importantly, this is not a drug-specific effect: it occurs with any cause of rapid significant weight loss, as documented in bariatric surgery literature. A 2023 JAAD review confirmed the primary driver is rate of fat loss, not the mechanism. Patients who lose weight gradually and maintain lean mass through resistance training and adequate protein tend to show less severe facial changes at equivalent weight loss percentages.
Are Ozempic before and after photos from real patients?
Some are, some are not — and the difference matters. Photos posted to social media (Reddit, TikTok, Instagram) are generally from real patients, but they lack clinical context: dose, duration, concurrent interventions, and selection bias (people who had dramatic results are far more likely to post). Clinic and telehealth provider photos are typically from actual patients who have signed a consent, but again, they represent the most successful outcomes in a practice’s patient population, not the average. Celebrity before-and-after comparisons circulated in tabloid media are almost always speculative — Ozempic use is frequently attributed without any confirmation, and other interventions (surgery, intensive fitness programs, dietary coaching) are rarely disclosed. For realistic expectations, the STEP 1 trial distribution in NEJM — where roughly 14% of participants did not even reach 5% weight loss and another 17% fell between 5–10% — is more useful than any curated photo collection.
When do you see Ozempic results in photos?
Most patients begin noticing a visible change in the mirror between weeks 8–16 — corresponding to the transition from the 0.5 mg titration dose to the 1 mg maintenance dose. Before-and-after photos taken at this stage (2–4 months) capture the period of most rapid visible change. The STEP 4 JAMA trial shows the steepest part of the weight loss curve falling in weeks 4–20, after which loss continues but more gradually. Patients who start taking weekly photos often notice changes in their neck and waist first, followed by the face and upper arms. The best clinical milestone for a meaningful before-and-after comparison is the 6-month mark, which aligns with dose stabilization, adaptation to the drug’s effects, and approximately 8–11% average loss per the Ghusn 2022 data.
Can you avoid Ozempic face with exercise?
Yes — resistance training is the most evidence-supported strategy for reducing facial volume loss during semaglutide therapy, though it cannot eliminate it entirely at large amounts of weight loss. The mechanism is indirect: resistance exercise preserves lean muscle mass throughout the body, including the muscular support structures underlying the face, and reduces the proportion of weight lost as fat-free mass. A 2022 analysis in Obesity (Wilding et al.) found that the semaglutide plus intensive behavioral therapy group — which included regular physical activity — showed better lean mass retention than semaglutide alone. The AACE/ACE obesity clinical practice guidelines recommend resistance training 2–3 times per week as standard adjunct care during GLP-1 pharmacotherapy. Combined with adequate dietary protein (1.2–1.5 g/kg/day per the STEP 3 dietary protocol) and gradual dose titration, resistance training gives patients the best realistic chance of achieving significant weight loss with minimal facial aging effect.
Find out if you qualify for Ozempic through WeightLossInjections.com. Our free intake takes under 3 minutes. A licensed provider reviews your history within 24 hours and, if appropriate, builds a personalized titration plan. Start your free intake →
This article is for educational purposes only and does not constitute medical advice. WeightLossInjections.com’s editorial team reviews all content quarterly; last medical review: April 2026. Weight loss results vary by individual; clinical trial averages represent population means, not guaranteed outcomes. Consult a licensed provider before starting any GLP-1 medication.
![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/04/hero_ozempic_c1_cost-1200x675.png)