Cheaper Alternatives to Ozempic in 2026: 8 Options Compared by Cost, Efficacy, and Access
Medically reviewed by WeightLossInjections.com Staff•Updated July 23, 2026•15 min readMedically reviewed
⤢
If you’re looking for a cheaper alternative to Ozempic in 2026, there are several options worth considering.
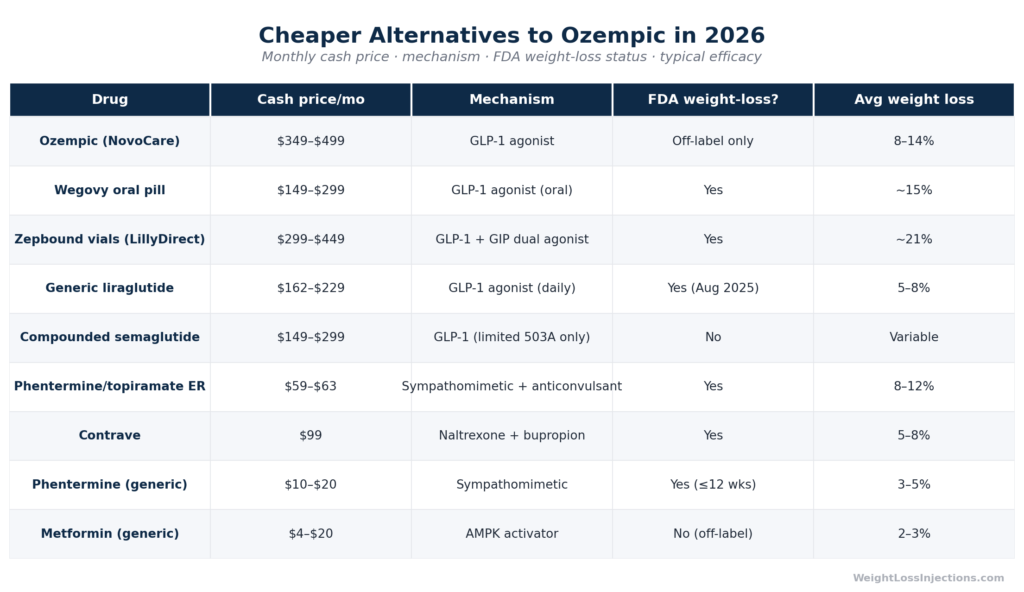
Ozempic’s cash price now runs about $499/month via NovoCare or $349/month through GoodRx — still steep for most patients. Cheaper alternatives span a wide range: generic liraglutide (GLP-1, ~$162–229/month with GoodRx), compounded semaglutide (legally restricted since the shortage resolved in early 2025, though a narrow pathway remains under 503A for individualized doses), Wegovy oral pill ($149–299/month via NovoCare), Zepbound vials ($299–449/month via LillyDirect), metformin (~$4–20/month), phentermine (~$10–20/month with GoodRx), Contrave ($99/month via manufacturer program), and phentermine/topiramate ER (~$59–63/month with GoodRx). “Cheaper” often means lower efficacy or different access conditions.
Ozempic’s list price sits at approximately $998 per month. In August 2025, Novo Nordisk cut the self-pay price through its NovoCare Pharmacy and a new GoodRx partnership to $499 per month, a significant reduction, but still $6,000 per year out of pocket. With a GoodRx introductory offer, new patients may pay $199–$349 for early fills, with ongoing fills running approximately $349/month at participating pharmacies, according to GoodRx pricing data.
Insurance coverage for weight loss remains inconsistent. The 2025 KFF Employer Health Benefits Survey found that only 43% of large employers (5,000+ workers) cover GLP-1s for weight loss, and several are pulling back coverage due to cost. Medicare does not cover Ozempic for weight loss; only 13 state Medicaid programs cover GLP-1s for obesity as of January 2026, per KFF Medicaid data.
The result: a large share of patients, particularly those without diabetes, are paying cash. This guide evaluates eight alternatives by actual 2026 prices, clinical efficacy, and practical access.
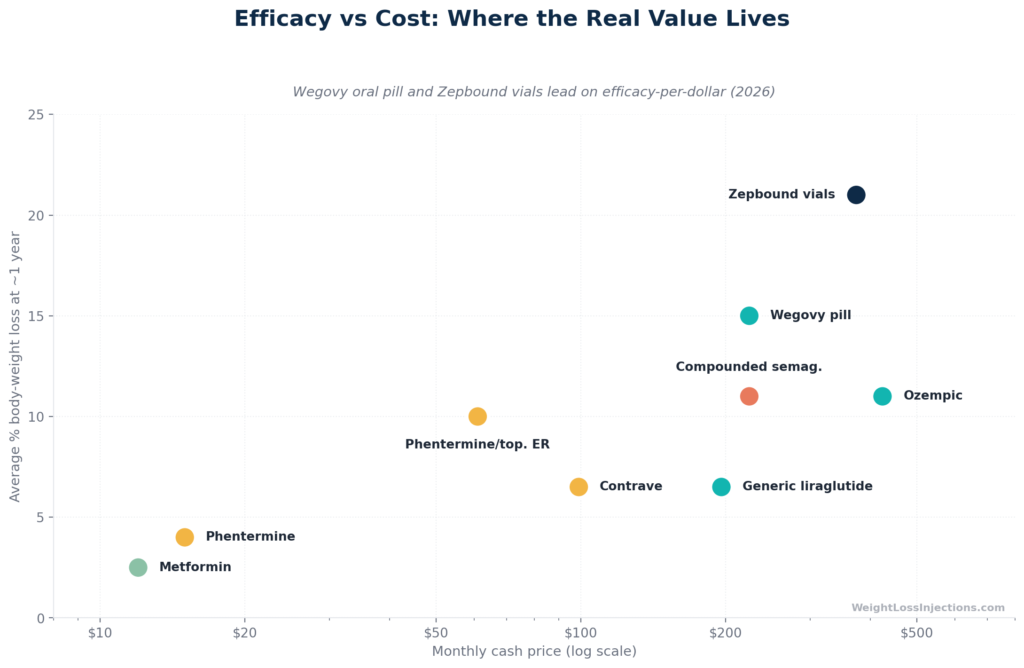
Our take at WeightLossInjections.com: “Cheaper” is a relative term that always needs a second variable, efficacy, access, or clinical fit. A medication that costs $20/month but produces 3% body weight loss is not the same as one that costs $300/month and produces 15%. We compare both dimensions here so you can make an informed choice with your provider.
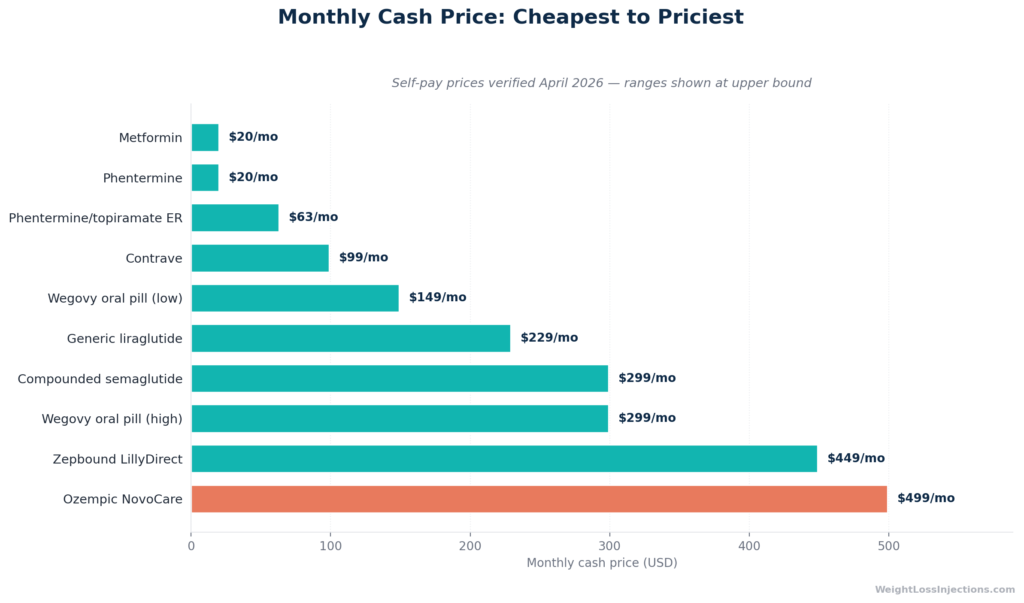
Cost ladder bar chart
#1: Wegovy oral pill — same drug, dramatically lower price
Monthly cost: $149–$299 via NovoCare Pharmacy, depending on dose Mechanism: GLP-1 receptor agonist (semaglutide) FDA-approved for weight loss: Yes
The most overlooked option in early 2026 is Novo Nordisk’s oral Wegovy pill, launched January 5, 2026. It contains the same active ingredient as Ozempic and Wegovy injections like semaglutide in a daily tablet format. Unlike Ozempic (which is not approved for weight loss), the oral Wegovy pill carries the full FDA weight-management indication.
Cash pricing via NovoCare: $149/month for 1.5 mg and 4 mg doses (the 4 mg introductory offer runs through August 31, 2026, then increases to $199/month); $299/month for 9 mg and 25 mg doses, per NovoCare pricing information. The injectable Wegovy pen is $199–$349/month through NovoCare, per Noom’s 2026 pricing summary.
Efficacy at the injectable 2.4 mg dose: the STEP 1 trial showed a mean 14.9% body weight reduction at 68 weeks in adults without diabetes versus 2.4% for placebo. For patients who prefer avoiding injections and qualify for weight management treatment, the oral pill at $149–$299/month is one of the most cost-effective GLP-1 pathways currently available.
Caveat: Coverage through insurance differs from the injectable. Verify your plan’s formulary before assuming the pill will be covered like the pen.
#2: Zepbound vials via LillyDirect — better efficacy, comparable cost
Monthly cost: $299–$449 via LillyDirect (vials); $1,086 list price for pre-filled pens Mechanism: GLP-1 + GIP dual receptor agonist (tirzepatide) FDA-approved for weight loss: Yes
If your goal is the greatest average weight loss per dollar spent, tirzepatide edges out semaglutide. In the SURMOUNT-1 trial, tirzepatide at 15 mg produced a mean 20.9% body weight loss at 72 weeks. Eli Lilly cut LillyDirect vial prices in December 2025: the 2.5 mg starting dose now runs $299/month; the 5 mg dose $399/month; all higher doses (7.5–15 mg) $449/month, per CNBC’s December 2025 report and Noom’s Zepbound cost guide.
Vials require drawing the dose with a syringe rather than using a pre-filled pen, a modest practical trade-off for $600+ in monthly savings versus retail pricing. Available through LillyDirect’s self-pay program with a valid prescription. For patients maintaining doses above 5 mg, Eli Lilly’s Zepbound Self Pay Journey Program (which requires refill within 45 days of previous delivery) maintains the $449 cap.
Note on Mounjaro: Mounjaro (tirzepatide) is FDA-approved for type 2 diabetes, not weight loss. Without insurance, its retail price runs $995–$1,069/month with GoodRx — significantly more than Zepbound vials for the same molecule. Cash-paying weight loss patients should use Zepbound, not Mounjaro, for the better self-pay price.
#3: Generic liraglutide — the first true generic GLP-1 for weight loss
Monthly cost: ~$162–229 for 3 pens (GoodRx, generic), compared to $810+ for brand Victoza/Saxenda Mechanism: GLP-1 receptor agonist FDA-approved for weight loss: Yes (Saxenda/generic liraglutide for chronic weight management)
August 28, 2025 was a milestone: Teva Pharmaceuticals received FDA approval for the first-ever generic GLP-1 indicated for weight loss, a generic to Saxenda (liraglutide injection), per Teva’s press release. Generic liraglutide is indicated for adults and adolescents (12+) with obesity or overweight with weight-related comorbidities, used with a reduced-calorie diet and increased physical activity.
GoodRx pricing for generic liraglutide injection (Victoza-equivalent, 3 pens of 18 mg/3 mL) runs approximately $162–$229/month, roughly 73–80% off brand pricing. This makes generic liraglutide among the most affordable FDA-approved GLP-1 options for weight loss currently available.
Efficacy: The LEADER trial established liraglutide’s cardiovascular risk-reduction profile in type 2 diabetes. For weight loss specifically, Saxenda trials (SCALE Obesity and Prediabetes) showed a mean ~8% body weight loss at one year at the 3 mg dose versus ~2.6% for placebo. That’s meaningfully less than Wegovy (14.9%) or Zepbound (20.9%), but the drug is FDA-approved for this indication and carries decades of clinical data.
Practical note: Liraglutide is a daily injection, versus semaglutide’s once weekly. Adherence data consistently shows that weekly injections have better compliance than daily. That’s a real-world consideration, not a minor footnote.
Also important: Liraglutide injection for diabetes (Victoza) is currently listed as being in shortage by the FDA. That status does not change the availability of the Saxenda/generic liraglutide weight-management formulation, but patients should verify availability at their pharmacy.
#4: Compounded semaglutide — where the law stands in 2026
Monthly cost: $149–$299 at telehealth platforms that currently offer it Mechanism: GLP-1 receptor agonist FDA-approved: No — compounded products are not FDA-approved
This section requires precision, because the legal landscape changed substantially in 2025 and has continued to evolve through April 2026.
What happened: The FDA declared the semaglutide injection shortage resolved on February 21, 2025. Enforcement discretion periods for state-licensed pharmacies (503A) ended April 22, 2025, and for outsourcing facilities (503B) ended May 22, 2025, per the FDA’s official shortage resolution announcement. A federal district court denied the compounding industry’s preliminary injunction on April 24, 2025, confirming the FDA’s authority.
Where things stand in April 2026: The FDA issued a clarifying statement on April 1, 2026 reminding compounders of the conditions required under sections 503A and 503B. Semaglutide and tirzepatide do not appear on the FDA’s drug shortage list or the 503B bulks list. Under 503A, a licensed pharmacy may still compound semaglutide for an individual patient if the prescriber documents a significant clinical difference (e.g., a medically necessary dose or formulation not available in any FDA-approved product). The FDA has stated it will not take action against a 503A compounder that fills four or fewer prescriptions of a semaglutide product per calendar month, per its April 2026 guidance. Large-scale “copy” compounding — the model used by most telehealth platforms during the shortage — is no longer a legally tenable operation at 503B outsourcing facilities. The FDA also issued 30 warning letters to telehealth companies in March 2026 for marketing compounded GLP-1s as equivalent to FDA-approved products, per Venable’s March 2026 regulatory analysis.
What this means for patients: Patients who were using compounded semaglutide during the shortage should transition to FDA-approved options. Some 503A pharmacies continue to compound semaglutide for patients with documented individual clinical need (e.g., specific non-standard doses). Availability is limited and inconsistent. Pricing at platforms still offering it ranges from $149–$299/month per recent market surveys, but access has tightened considerably.
WeightLossInjections.com editorial note: We do not recommend seeking compounded semaglutide from telehealth platforms that are marketing it as equivalent to Ozempic or Wegovy. That practice is specifically what FDA’s March 2026 warning letters target. If you and your prescriber believe a compounded formulation is medically necessary for your individual clinical situation, that conversation should happen with your provider — not through mass-market telehealth funnels.
Our Top 3 · August 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Monthly cost: $4–$20 (generic, GoodRx), per GoodRx metformin pricing Mechanism: Activates AMPK; improves insulin sensitivity; mild appetite suppression FDA-approved for weight loss: No (approved for type 2 diabetes)
Metformin is the baseline against which all weight-loss drug costs should be measured. At $4/month at Walmart for a 30-day supply (or $8.65 with GoodRx for 180 tablets of 1,000 mg), its cost-per-outcome ratio is unmatched for a specific patient population.
Efficacy for weight loss is real but modest. The Diabetes Prevention Program (DPP), a landmark NIH trial, found that metformin-treated participants lost a mean 2.1 kg over the initial 2.8 years — significantly less than the intensive lifestyle group’s 5.6 kg, but with one important distinction: the weight loss in the metformin group was maintained over 10+ years, while the lifestyle intervention group progressively regained weight, per a Cleveland Clinic Journal of Medicine review. Roughly 30% of participants on metformin lost more than 5% of their body weight in the first year.
This is not a drug to prescribe for dramatic weight loss. It is the appropriate starting point for patients with type 2 diabetes, prediabetes, or significant insulin resistance — particularly those with BMI ≥ 35 or younger patients — and it can be meaningfully combined with GLP-1s or lifestyle programs. Its cardiovascular safety data spanning decades is a clinical advantage that no newer drug can yet match.
Best fit: Patients with T2D or prediabetes who cannot afford GLP-1s; as combination therapy alongside a GLP-1.
#6: Phentermine and phentermine/topiramate ER (Qsymia)
Monthly cost — phentermine alone: $10–$20/month with GoodRx, per GoodRx phentermine data Monthly cost — phentermine/topiramate ER (Qsymia generic): $59–$63/month with GoodRx, per GoodRx phentermine/topiramate data Mechanism: Sympathomimetic (phentermine); anticonvulsant/carbonic anhydrase inhibitor (topiramate) FDA-approved for weight loss: Yes (phentermine: ≤12 weeks; phentermine/topiramate ER: chronic management)
Phentermine alone is one of the oldest FDA-approved weight loss drugs, approved since 1959. As a generic, it runs $10–$20/month, making it among the cheapest prescription options available. However, it’s approved only for short-term use (≤12 weeks), carries cardiovascular contraindications (including uncontrolled hypertension, coronary artery disease, and hyperthyroidism), and is classified as a Schedule IV controlled substance.
Phentermine/topiramate extended-release (Qsymia), now available as a generic at $59–$63/month with GoodRx, is a meaningfully different proposition. Phase III CONQUER and EQUIP trials found mean weight loss of ~12–14% of body weight at 56 weeks at the maximum dose (15/92 mg), with 67–70% of patients losing ≥5% of body weight, per PMC review of the trials. A two-year SEQUEL extension confirmed sustained weight loss of ~10–12% at 108 weeks.
At $59–$63/month, phentermine/topiramate ER offers one of the best efficacy-to-cost ratios of any FDA-approved obesity medication currently available. Key limitations: contraindicated in pregnancy (topiramate is teratogenic, requiring negative pregnancy testing before and during treatment); cognitive side effects (word-finding difficulty, memory); can increase heart rate; patients with glaucoma should not use it.
Best fit: Patients who need meaningful weight loss at minimal cost, have no cardiovascular contraindications or reproductive safety concerns, and want an FDA-approved, evidence-backed option.
#7: Contrave (naltrexone/bupropion)
Monthly cost: $99/month via manufacturer’s CurAccess™ program; $199–$741 at retail pharmacies; $199 with GoodRx, per GoodRx Contrave pricing and Noom’s Contrave cost guide Mechanism: Opioid antagonist (naltrexone) + antidepressant (bupropion); acts on hypothalamic and mesolimbic appetite and reward pathways FDA-approved for weight loss: Yes (chronic weight management)
Contrave combines naltrexone (8 mg) and bupropion (90 mg) in an extended-release formulation. The COR trial series, four 56-week phase III randomized controlled trials enrolling 4,536 patients, established its efficacy: at the 32 mg naltrexone / 360 mg bupropion dose, patients lost 5.4–8.2% of body weight versus 1.2–4.9% for placebo, with 42–65% achieving ≥5% weight loss, per PMC review of the COR trials.
That efficacy is lower than GLP-1s, but at $99/month through the manufacturer’s CurAccess™ program (available to cash-paying patients including Medicare, Medicaid, and TRICARE beneficiaries), it’s one of the most accessible FDA-approved options for patients who cannot use GLP-1s (prior opioid dependence treated with buprenorphine, for example, is a contraindication for naltrexone; seizure disorders are a contraindication for bupropion).
Key considerations: Contraindicated in patients on opioid medications (the naltrexone component will precipitate withdrawal), patients with seizure disorders, patients using MAOIs, and patients with uncontrolled hypertension. Bupropion carries an FDA boxed warning for suicidal thoughts in young patients.
#8: Rybelsus (oral semaglutide for diabetes)
Monthly cost: ~$850–950 with GoodRx/SingleCare; $997.58 list price; $10 with commercial insurance + Novo savings card Mechanism: GLP-1 receptor agonist (oral semaglutide) FDA-approved for weight loss: No (approved for type 2 diabetes)
Rybelsus is an oral semaglutide tablet approved for type 2 diabetes. It is not approved for weight loss — that’s the Wegovy pill. Without strong insurance coverage, it costs nearly as much as Ozempic (~$850–998/month), placing it in the “same active ingredient, similar price, no weight-loss indication” category. With commercial insurance and the Novo Nordisk savings card, it can run as low as $10/month, which is genuinely cheap, but only accessible to patients with T2D and qualifying insurance.
For weight loss patients paying cash, the oral Wegovy pill ($149–$299/month via NovoCare) is a strictly superior option: same mechanism, lower self-pay price, and an actual weight-loss indication. Rybelsus belongs in this list mainly to clarify the confusion between it and the Wegovy pill.
Telehealth is the dominant channel for self-pay GLP-1 access in 2026, but the options have shifted since the compounded semaglutide boom of 2023–2024.
Legitimate lower-cost pathways:
NovoCare Pharmacy (Novo Nordisk): Self-pay patients can access Wegovy injection ($199–$349/month) and Wegovy pill ($149–$299/month) or Ozempic ($499/month) through Novo’s direct pharmacy or telehealth partners. Requires a valid prescription for the labeled indication.
LillyDirect (Eli Lilly): Self-pay patients with a valid on-label Zepbound prescription can access single-dose vials ($299–$449/month) or the new multi-dose KwikPen (same pricing). Available for home delivery or pickup at partner Walmart pharmacies.
Patient assistance: Novo Nordisk’s Wegovy and Ozempic savings cards bring commercially insured patients to as low as $25/month when plans cover the drug. Eli Lilly’s Zepbound Savings Card similarly covers commercially insured patients. Eligibility requires commercial insurance (not Medicare or Medicaid).
GoodRx and discount cards: Generic liraglutide at $162–$229/month with GoodRx represents one of the most straightforward access pathways for an FDA-approved GLP-1 weight-loss medication.
When evaluating a telehealth provider, ask:
Is the medication FDA-approved, or compounded? (Both are legal in the right circumstances — but they are not the same.)
Who is prescribing? A licensed physician, NP, or PA in your state must be identified.
What’s included beyond medication? Dose adjustments, lab monitoring, provider messaging.
Is pricing per month, or locked into a multi-month commitment?
Our take at WeightLossInjections.com: At WeightLossInjections.com, patients working with our licensed providers start at [$X/month] all-in, which includes [service detail]. That price covers ongoing provider access, dose adjustments, and support — not just the medication. We use FDA-approved medications. We can walk you through eligibility in a free 3-minute intake.
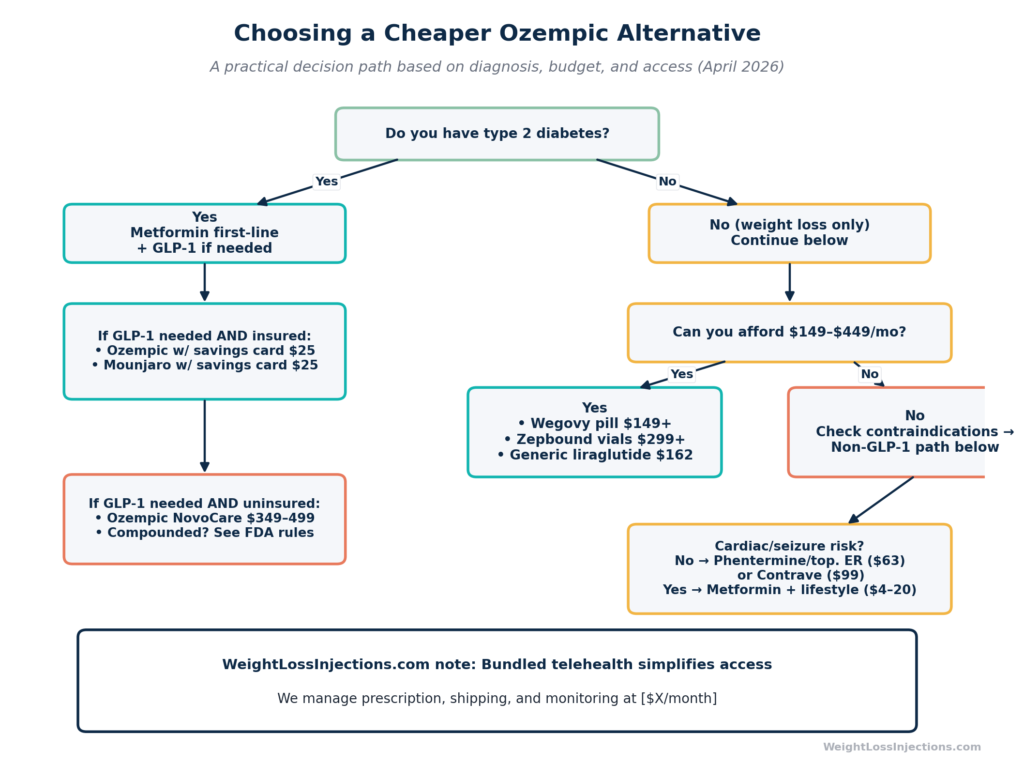
Decision flowchart
Frequently asked questions
It depends on the context. The FDA resolved the semaglutide shortage in February 2025, ending the large-scale compounding that defined 2022–2024. As of April 2026, 503B outsourcing facilities cannot compound semaglutide copies at scale. Under 503A, a state-licensed pharmacy can still compound semaglutide for an individual patient if a prescriber documents a significant clinical difference from available FDA-approved products — but the FDA has stated it will only exercise enforcement discretion for compounders filling four or fewer prescriptions of that product per calendar month. Mass-market “compounded Ozempic” marketed as a generic substitute is not a legally compliant product in 2026, per the FDA’s April 1, 2026 guidance.
As of April 2026, generic liraglutide injection (~$162–229/month with GoodRx, per GoodRx data) is the most affordable FDA-approved GLP-1 specifically indicated for weight loss — following Teva’s August 2025 approval. The oral Wegovy pill at $149/month (starting dose, via NovoCare) is comparably priced and has stronger weight-loss efficacy data.
At Walmart, generic metformin starts at $4/month, compared to Ozempic’s $349–499/month self-pay price. That’s 98–99% cheaper. However, efficacy is vastly different: Ozempic produces 8–14% body weight loss at therapeutic doses; metformin produces ~2–3% in most populations. Metformin is appropriate as a starting therapy for patients with T2D, prediabetes, or insulin resistance, not as a weight-loss drug in patients without metabolic indications.
Coverage varies by drug and indication. Ozempic is broadly covered for type 2 diabetes; coverage for weight loss is rare. Wegovy for weight management is covered by a growing minority of employer plans, 43% of large employers (5,000+ workers) covered GLP-1s for weight loss in 2025, per KFF, though several are scaling back. Medicare does not cover weight-loss GLP-1s unless the indication is cardiovascular risk reduction (Wegovy) or sleep apnea (Zepbound). Metformin is universally covered for T2D. Phentermine/topiramate ER and Contrave have inconsistent commercial coverage; the manufacturer’s cash program for Contrave ($99/month) is often more accessible than waiting for insurance.
Both contain semaglutide, but Ozempic is FDA-approved for type 2 diabetes (maximum 2.0 mg weekly) while Wegovy is FDA-approved for chronic weight management (maximum 2.4 mg injection weekly, or a daily pill with different dosing). The higher dose in Wegovy, combined with its specific weight-loss indication, produces slightly more average weight loss than Ozempic at its 2.0 mg ceiling. For patients paying cash, the Wegovy pill at $149–299/month through NovoCare is often cheaper than Ozempic via NovoCare at $499/month and carries the appropriate label. See our Ozempic vs. Wegovy guide for the full comparison.
Key sources
FDA — GLP-1 compounding policies as national supply stabilizes, April 2026 — fda.gov
Novo Nordisk — Wegovy price guide, NovoCare Pharmacy — novocare.com
Eli Lilly — Zepbound vial price reduction, December 2025 — CNBC
Teva — FDA approval of generic Saxenda (liraglutide), August 28, 2025 — ir.tevapharm.com
Noom — Wegovy cost without insurance, 2026 — noom.com
Noom — Zepbound cost without insurance, 2026 — noom.com
This article is for educational purposes only and is not a substitute for medical advice. WeightLossInjections.com’s medical team reviews content quarterly; last medical review: April 2026. Consult a licensed provider before starting or switching any weight-loss medication.
![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/04/hero_ozempic_c1_cost-1200x675.png)