![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/05/hero_zepbound_c5_lifestyle-1200x675.png)
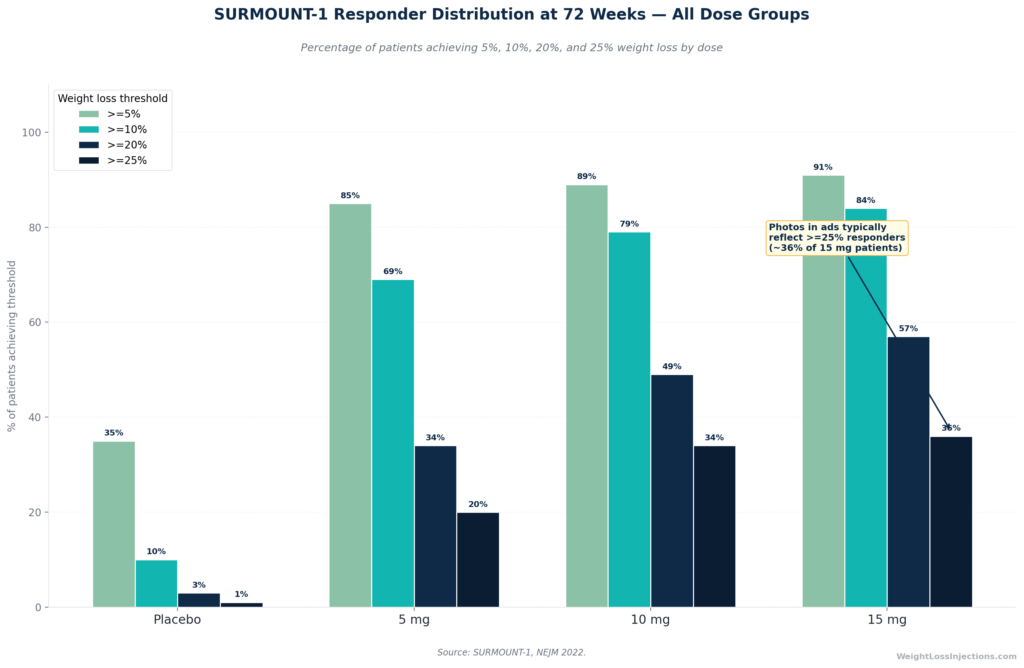
SURMOUNT-1 Responder Distribution at 72 Weeks
At 72 weeks on Zepbound 15 mg, the average patient loses 20.9% of body weight, roughly 48 lbs from a 230-lb starting weight. That is the clinical average. The dramatic before-and-after photos circulating online typically depict patients from the top ~36% of responders, those who lost 25% or more.
This article pairs the published SURMOUNT trial data with a transparent breakdown of what physical changes look like month by month, what happens to the body beyond the scale, and what the “after the after” picture looks like if you stop taking Zepbound. All images in this article are data charts, no stock photos, no fabricated before-and-after images.
What “Before and After” Photos Actually Represent, and What They Don’t
Walk into any search engine and type “Zepbound before and after.” You will find photos of extraordinary physical transformations: faces sharply defined, waistlines dramatically reduced, clothing sizes halved. These images are real in the sense that they reflect actual results achieved by actual patients. But they represent a specific slice of the patient population, not the average, and not the typical.
The marketing math is worth understanding. In SURMOUNT-1, the pivotal 72-week Phase 3 trial published in the New England Journal of Medicine, 57% of patients on the 15 mg dose lost 20% or more of their body weight. That is remarkable. But the threshold that produces visually dramatic photos, the kind where even strangers notice, typically requires 25% or more body weight reduction. Per the same NEJM 2022 data, approximately 36% of 15 mg patients reached that level. That means the before-and-after photos circulating in ads and on social media are drawn disproportionately from the top third of responders.
This matters for expectation-setting, not because 20% body weight loss is unimpressive, it absolutely is not, but because patients who see the top-third photos and expect a top-third result have been given only part of the picture. The average Zepbound patient loses real, clinically significant weight. The average Zepbound patient also does not look like a pharmaceutical advertisement after 18 months.
There is also a time-frame problem with circulating photos. Zepbound’s titration schedule means the maximum dose of 15 mg is not reached until at minimum week 20 of treatment. Most dramatic transformation photos represent 12–18+ months of treatment at maximum tolerated dose, not 3 or 6 months. Photos labeled “results in 3 months” almost always reflect patients on a 5–10 mg dose range, which produces 15–19% average loss at 72 weeks, still meaningful, but not what 15 mg achieves over a longer window.
The purpose of this article is to give you the complete picture: what trial data says about the average, what the physical transformation actually looks and feels like, and how to contextualize the dramatic cases you will encounter everywhere online.
SURMOUNT-1 Real Data: Averages, Distribution, and What “Typical” Means
The foundational dataset for any Zepbound before-and-after discussion is SURMOUNT-1, published in the New England Journal of Medicine in 2022 by Jastreboff et al. This was a randomized, double-blind, placebo-controlled Phase 3 trial enrolling 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, excluding type 2 diabetes.
The Headline Numbers at 72 Weeks
| Dose | Average % Weight Loss | ≥5% Responders | ≥10% Responders | ≥20% Responders |
|---|---|---|---|---|
| Placebo | −3.1% | 35% | ~10% | 3% |
| 5 mg | −15.0% | 85% | 69% | 34% |
| 10 mg | −19.5% | 89% | 79% | 49% |
| 15 mg | −20.9% | 91% | 84% | 57% |
Source: SURMOUNT-1, NEJM 2022, Jastreboff et al.
The average weight of SURMOUNT-1 participants at baseline was approximately 231 lbs (105 kg). At 15 mg, the average loss was 20.9%, approximately 48 lbs, reducing the average patient from 231 lbs to around 183 lbs. That is a clinically profound change. It exceeds what most long-term behavioral interventions achieve, and it approaches or matches outcomes from certain bariatric procedures in some patient categories.
Concrete Starting-Weight Examples
Because percentage loss reads differently depending on where you start, here is the same data expressed in pounds:
| Starting Weight | 5 mg Avg (−15%) | 10 mg Avg (−19.5%) | 15 mg Avg (−20.9%) |
|---|---|---|---|
| 200 lbs | −30 lbs | −39 lbs | −42 lbs |
| 225 lbs | −34 lbs | −44 lbs | −47 lbs |
| 250 lbs | −37 lbs | −49 lbs | −52 lbs |
| 275 lbs | −41 lbs | −54 lbs | −58 lbs |
| 300 lbs | −45 lbs | −59 lbs | −63 lbs |
Calculated by applying SURMOUNT-1 mean percentage changes to common starting weights. Individual results vary; these are population averages, not guaranteed outcomes. Source: SURMOUNT-1, NEJM 2022.
What SURMOUNT-1 Looked Like for Patients With Type 2 Diabetes
SURMOUNT-1 enrolled non-diabetic patients. For patients with type 2 diabetes, the relevant data comes from SURMOUNT-2, published in The Lancet in 2023. At 15 mg and 72 weeks, T2D patients lost an average of 14.7% of body weight (versus 3.2% on placebo) — still clinically significant, but approximately 6 percentage points less than non-diabetic patients. The ACC SURMOUNT-2 summary notes that 83% of T2D patients on 15 mg lost ≥5% of body weight, and HbA1c was reduced by 2.08 percentage points, with 49% achieving normoglycemic levels below 5.7%. The visual and physical transformation is real for T2D patients — it just runs at a somewhat lower magnitude.
For a full breakdown of clinical results by dose and endpoint, see our companion article on Zepbound weight loss results.
Typical Trajectory Month by Month: When Do You See Changes?
Understanding the timeline is as important as understanding the endpoints. Zepbound’s FDA-labeled titration schedule means patients spend the first 20 weeks climbing through the dose ladder, not at maximum therapeutic dose. This shapes what a before-and-after photo taken at month 3 represents versus one taken at month 12 or 18.
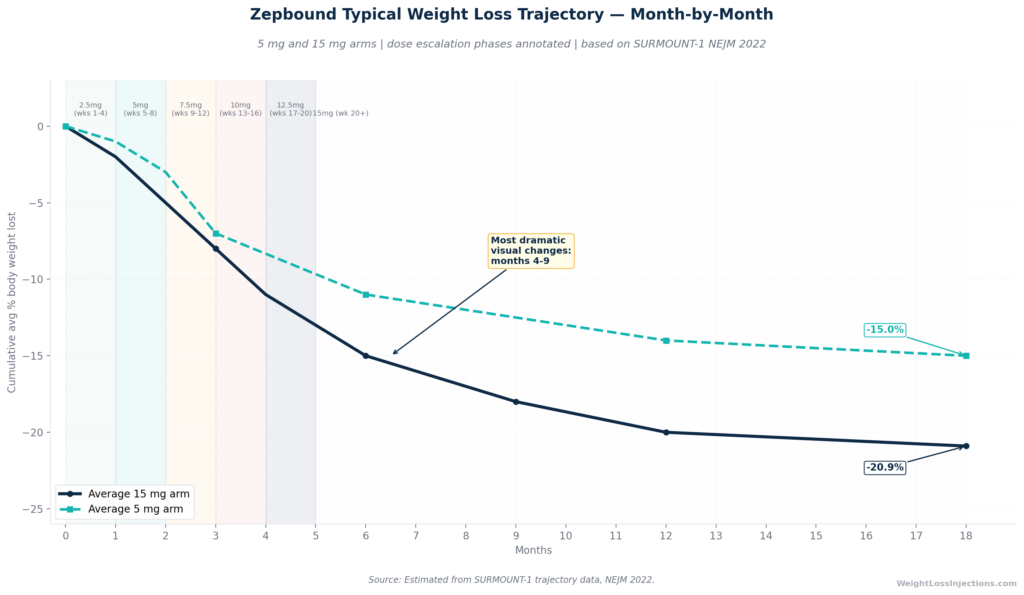
Zepbound Typical Weight Loss Trajectory: Month-by-Month Curve
Weeks 1–4: The Invisible Before
Week 1 through week 4, patients take the 2.5 mg initiation dose. Per the Zepbound prescribing information, this dose is explicitly a tolerability step, it brings tirzepatide plasma levels into the system and allows the gastrointestinal tract to adapt to the drug’s gastric-emptying effect. Most patients see little change on the scale in this phase.
What patients do report, often within days, is a reduction in what many describe as “food noise”, the persistent background mental pull toward eating. Tirzepatide’s dual mechanism as a GIP and GLP-1 receptor agonist begins dampening both appetite and reward-driven eating signals quickly, even before weight loss is measurable. The “before” visually looks unchanged at week 4. Biologically, the drug has begun working.
Steady-state plasma concentrations are not reached until approximately 4 weeks of consistent once-weekly dosing per the Zepbound prescribing information, which means the full pharmacological effect of any given dose is not present until the end of each 4-week dose phase.
Months 2–3: The First Visible Changes
Dose escalation to 5 mg, then 7.5 mg through months 2 and 3 begins producing accelerating weight loss. For a 250-lb patient, losing 7–10% of starting weight by month 3 translates to 17–25 lbs. This is where the first physical changes typically become visible, not necessarily to others, but to the patient in the mirror and in their clothing.
Where patients notice change first is instructive. SURMOUNT-1 measured a total waist circumference reduction of −19.4 cm (~7.6 inches) at 72 weeks. The majority of that visceral fat reduction begins accumulating in months 2–6. A patient who loses 15–20 lbs notices it first in the face and neck (jawline definition, reduction of fullness under the chin), in the waistband of pants, and in how sleeves and collars fit. The scale may say 20 lbs lost; clothing makes it look like more, because visceral and subcutaneous abdominal fat is reducing faster than overall body mass.
See our Zepbound dosage chart for a full breakdown of the escalation schedule and what to expect at each dose step.
Months 4–6: The Most Visually Dramatic Phase
This is the phase most likely to be captured in before-and-after photos. Patients are at 10–15 mg, the dose range producing the most accelerating loss. Cumulative loss at month 6 typically ranges from 14–18% at the 15 mg arm trajectory, translating to 32–42 lbs from a 230-lb starting weight.
This is where external social recognition begins. Coworkers comment. Clothing sizes change. Energy and physical mobility often improve markedly as joint load decreases. For patients prescribed Zepbound for obstructive sleep apnea, this phase frequently shows the most dramatic OSA improvements: SURMOUNT-OSA found that 42% of tirzepatide patients (no PAP arm) and 50% (PAP arm) no longer had moderate-to-severe OSA at 52 weeks, compared to 16% and 14% on placebo.
Importantly, the first side effects also tend to peak in this phase as dose escalation continues. Nausea, constipation, and GI discomfort, reported by 56% of pooled Zepbound patients versus 30% of placebo in FDA prescribing information data, typically correlate with each new dose step. These are generally transient and manageable, but they are part of the real before-and-after experience. See our dedicated guide to Zepbound side effects in week 1 for what to expect during each escalation.
Months 7–12: Consolidating the Transformation
By month 7–12, most patients are at their maximum tolerated dose and approaching the plateau that SURMOUNT-1 data shows near 60–72 weeks. Average cumulative loss reaches 20.9% at 72 weeks for the 15 mg arm, and the physical transformation is at or near its maximum on medication.
Lab values tell the story the mirror doesn’t. SURMOUNT-1 documented: systolic blood pressure reduced by 7.2 mmHg versus 1.0 mmHg on placebo; fasting insulin reduced by 54.7% versus 11.3% on placebo; triglycerides reduced by 24.8% versus 5.7% on placebo. These are the metabolic “afters” that do not appear in any photo.
Beyond 12 Months: Maintenance and the 3-Year Picture
The 3-year extension of SURMOUNT-1 in the prediabetes subgroup, published in the New England Journal of Medicine in 2025, found a mean weight reduction of −19.7% maintained at 176 weeks (approximately 3.4 years) on continued treatment. Weight loss rate slows considerably after 60–72 weeks as the body reaches a new defended set point. This is normal physiology, not treatment failure. The plateau at roughly 20–21% loss is the expected steady-state outcome for most patients on 15 mg. Expecting continued rapid loss after 18 months on the same dose is not supported by the evidence.
Beyond the Scale: Body Composition — What Actually Changes
The before-and-after story that almost never appears in photos is the body composition story. Weight on a scale is not a precise measure of what has changed. SURMOUNT-1 measured multiple markers simultaneously at 72 weeks, and the picture is considerably richer than any single number.
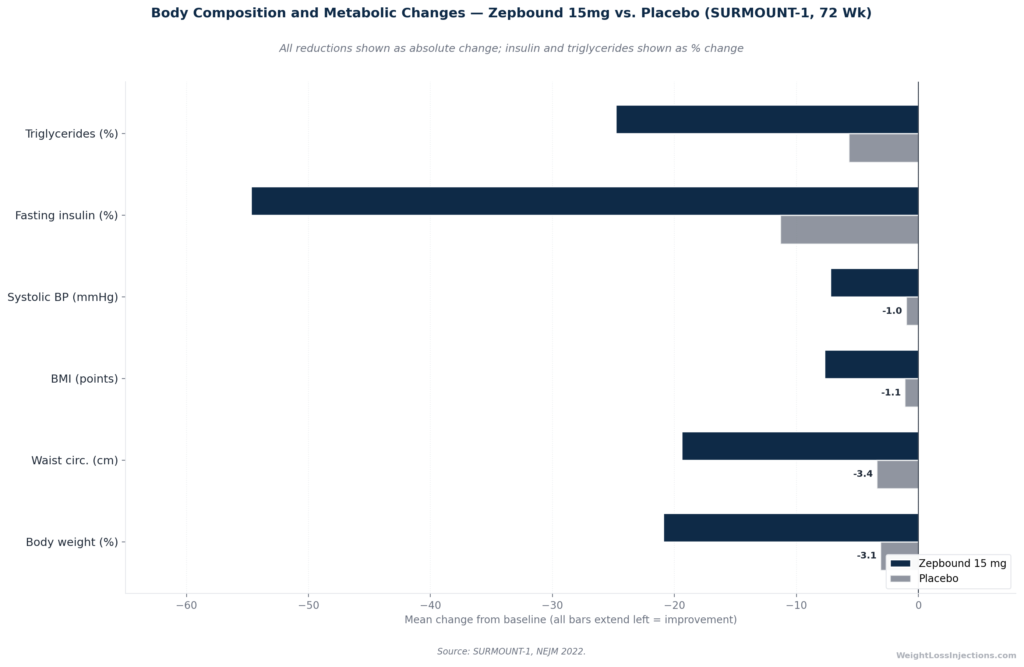
Body Composition and Metabolic Changes: Zepbound 15 mg vs. Placebo at 72 Weeks (SURMOUNT-1)
The Full Metabolic “After”
The table below summarizes what SURMOUNT-1 measured beyond body weight at 72 weeks on 15 mg versus placebo:
| Measurement | Zepbound 15 mg | Placebo | Clinical Significance |
|---|---|---|---|
| Body weight | −20.9% | −3.1% | Approaches bariatric surgery outcomes in top responders |
| Waist circumference | −19.4 cm (~7.6 in) | −3.4 cm | Visceral fat reduction; reduced cardiometabolic risk |
| BMI | −7.7 points | −1.1 points | Many patients shift to a lower obesity class |
| Systolic blood pressure | −7.2 mmHg | −1.0 mmHg | Clinically meaningful for hypertensive patients |
| Fasting insulin | −54.7% | −11.3% | Major improvement in insulin sensitivity |
| Triglycerides | −24.8% | −5.7% | Improved lipid profile |
Source: SURMOUNT-1, NEJM 2022, Jastreboff et al.
A waist circumference reduction of nearly 8 inches is not a cosmetic change. It represents a major reduction in visceral adipose tissue, the fat depot most closely linked to insulin resistance, cardiovascular disease risk, and systemic inflammation. Patients who look at before-and-after photos see clothing fit. A cardiologist sees this data.
Lean Mass: The Body Composition Tradeoff
There is one body composition reality that rarely appears in Zepbound promotional content: not all weight lost on Zepbound is fat. The SURMOUNT-1 DXA body composition substudy found that approximately 25% of total weight lost was lean mass (muscle and other non-fat tissue) without structured resistance training. With resistance training incorporated, this proportion can drop to approximately 15%.
This has real-world consequences. A patient who loses 50 lbs on Zepbound but neglects resistance training may lose roughly 12–13 lbs of lean mass alongside 37–38 lbs of fat. That lean mass loss, if it is predominantly muscle, affects resting metabolic rate and long-term weight maintenance. It is one reason why SURMOUNT-3, published in Nature Medicine in 2023, which combined Zepbound with intensive lifestyle intervention including exercise, produced total weight loss of −24.3% from baseline, superior to medication alone, and likely with better lean mass retention. Structured resistance training during treatment is not optional for optimal body composition outcomes; it is a meaningful modifier of what your “after” looks like in terms of metabolic health and muscle definition.
“Zepbound Face” — What Facial Changes Actually Reflect
A term that appears in patient communities is “Zepbound face”, the visible hollowing of the face, defined cheekbones, and reduced fullness under the chin that occurs during significant weight loss. This is not unique to Zepbound; it occurs with any substantial weight loss. The face has relatively little visceral fat, so facial changes tend to track closely with overall percentage body weight loss.
At 10–15% total body weight reduction, most patients see noticeable facial definition changes. At 20%+ loss, facial transformation is typically pronounced. For a patient starting at 230 lbs, this means visible facial change becomes significant at roughly 23–46 lbs lost, a range that most SURMOUNT-1 patients achieve well before the 72-week endpoint.
The honest framing: “Zepbound face” is what happens when a person who carried excess weight for years loses a medically significant amount of it. It reflects real physiological change. Whether that change is perceived as dramatic or natural depends partly on starting weight, facial fat distribution, age, and skin elasticity, none of which the drug controls.
Clothing Size Math: What Weight Loss Translates to in Practical Terms
Patients frequently ask how many clothing sizes they will drop. The relationship between pounds lost and size change is not precise, it varies by brand, cut, body fat distribution, and starting size, but general estimates from garment industry and body measurement data provide reasonable anchors:
- Each dress or pants size typically spans 10–15 lbs in body weight and 1–1.5 inches in waist circumference, though this varies substantially by manufacturer and body type.
- Given SURMOUNT-1’s average waist circumference reduction of −19.4 cm (approximately 7.6 inches) at 72 weeks on 15 mg, an average patient might expect to drop 4–6 pants sizes in waist circumference terms — though height, body shape, and fat distribution all modify this estimate.
- A patient losing 47 lbs from a 225-lb starting weight (the 15 mg average) can generally expect to drop 2–4 clothing sizes, with more if loss is concentrated in the abdomen and hips.
The patients shown in dramatic before-and-after content typically started at higher BMIs where the same percentage loss produces larger absolute changes, and they often lost 55–65+ lbs — which translates into more conspicuous size changes.
Our Top 3 · July 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
The Plateau: Why Weight Loss Slows After 72 Weeks
SURMOUNT-1 showed that the rate of weight loss decelerates markedly after approximately 60–72 weeks on maximum dose. This is not a treatment failure; it is a physiological defense mechanism. As body weight decreases, resting energy expenditure decreases, and the body’s defended set point adapts. The result is that the final maintained weight at continued maximum dose represents a new lower equilibrium — not the beginning of a further downward trend.
The 3-year SURMOUNT-1 extension data in NEJM 2025 shows this clearly: at 176 weeks, the prediabetes subgroup maintained an average of −19.7% from baseline. This is essentially the same level achieved at 72 weeks, confirming that continued treatment preserves but does not further extend average loss for most patients beyond the first 18 months. Patients who expect continued dramatic loss after a 72-week plateau have been misled by the early-phase trajectory.
“After the After” — What Happens When You Stop Zepbound
This is the question that most before-and-after articles never answer. SURMOUNT-4, published in JAMA in 2023, answered it directly with a randomized withdrawal design.
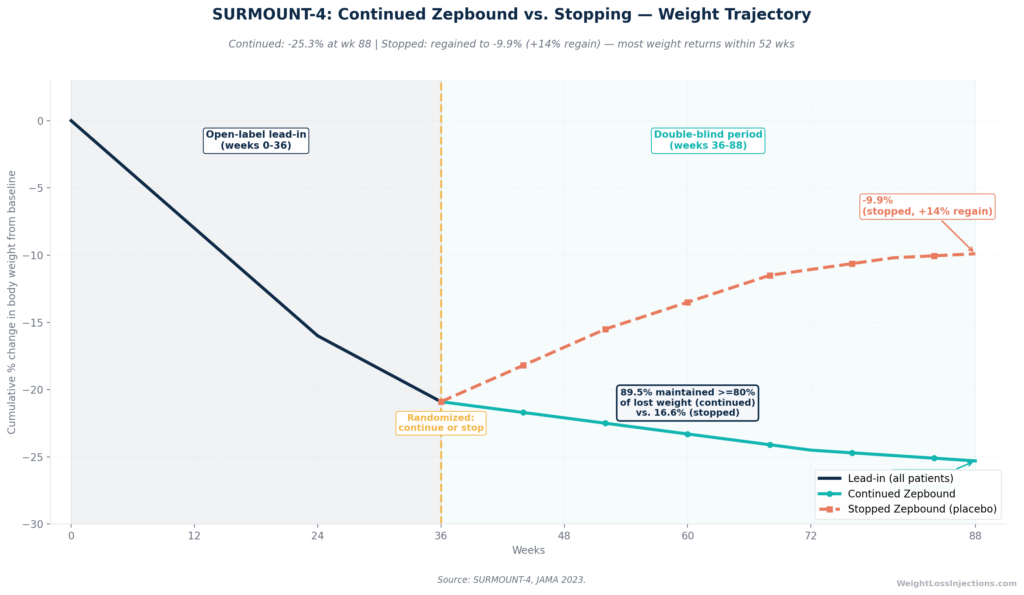
SURMOUNT-4 Weight Trajectory: Continued Zepbound vs. Stopping
The SURMOUNT-4 Findings
In SURMOUNT-4, 670 patients who had already lost an average of 20.9% of body weight during a 36-week open-label tirzepatide lead-in were randomized to either continue Zepbound or switch to placebo for 52 more weeks. The results were unambiguous:
- Continued Zepbound: Additional −5.5% weight loss, reaching −25.3% from original baseline. 89.5% of patients maintained ≥80% of their initial weight loss.
- Switched to placebo (stopped Zepbound): +14.0% weight regain from the week-36 weight, ending at −9.9% from original baseline. Only 16.6% maintained ≥80% of their initial weight loss.
Source: SURMOUNT-4, JAMA 2023; PubMed abstract, SURMOUNT-4
This means the “before and after” photos taken at peak Zepbound treatment are not permanent in the absence of continued medication. Stopping Zepbound typically reverses most of the weight lost within 12 months. This is not a product failure; it reflects the chronic nature of obesity as a disease. Just as stopping a blood pressure medication allows blood pressure to return toward pre-treatment levels, stopping an anti-obesity medication allows weight to return toward its prior defended set point.
The clinical and practical implication is significant: the “after” photo requires ongoing treatment to remain accurate. Patients who plan to use Zepbound as a finite course and then maintain results through lifestyle alone should understand that only 16.6% of those who stopped Zepbound in SURMOUNT-4 maintained ≥80% of their weight loss at the end of the withdrawal period.
Lifestyle Factors That Drive “Dramatic” Results, and Those That Don’t
Within the trial data, several factors reliably separate average responders from top-third responders. Understanding these allows a realistic appraisal of what “dramatic” before-and-after outcomes require.
Dose Achieved
The single largest predictor of outcome magnitude is dose. Average loss at 5 mg is 15%; at 15 mg, it is 20.9%. These are not trivial differences. The gap in ≥20% responders (34% vs. 57%) is even larger. Most patients target 15 mg, but GI tolerability limits some patients to 10 mg or below. The visual outcome difference between a patient who tolerates 15 mg and one who can only tolerate 10 mg is real and clinically significant. Tolerability strategies, slower escalation, dietary adjustments, antiemetic support, are worth pursuing precisely because reaching maximum tolerated dose has a direct impact on transformation magnitude.
Structured Dietary Intervention
SURMOUNT-3, in Nature Medicine 2023, combined a 12-week intensive behavioral intervention (including caloric restriction and exercise) with tirzepatide and produced total weight loss of −24.3% from the program start, compared to −18.4% for standard-counseling tirzepatide patients. The lifestyle component added roughly 6 percentage points of additional loss and likely improved the lean mass picture. The food environment matters; Zepbound is a powerful tool, but it works best when paired with structured dietary strategy.
A high-protein dietary pattern is particularly relevant to body composition. Adequate protein intake, approximately 1.2–1.6 g per kilogram of body weight per day, reduces the proportion of lean mass lost during the drug-driven caloric deficit. For a 230-lb (105 kg) patient, that is 125–170 grams of protein daily. Reducing ultra-processed food intake removes calorie-dense, low-satiety foods that can partially offset Zepbound’s appetite suppression.
Resistance Training
As noted above, the DXA substudy data from SURMOUNT-1 indicates roughly 25% of lost weight is lean mass without resistance training, dropping to approximately 15% with structured training. For a patient losing 50 lbs, that is the difference between losing ~12 lbs of muscle versus ~7.5 lbs. Preserving lean mass during weight loss is not just cosmetic — it supports resting metabolic rate, functional strength, and long-term weight maintenance capacity.
Adherence and Missed Doses
Tirzepatide has a half-life of approximately 5–6 days, meaning once-weekly dosing maintains relatively stable plasma concentrations. However, consistent adherence matters. Per the Zepbound prescribing information, if a dose is missed and it has been more than 4 days (96 hours), that dose should be skipped and the regular schedule resumed. Frequent dose gaps disrupt steady-state concentrations and reduce cumulative efficacy. Patients in SURMOUNT-1 received meticulous adherence support in a controlled trial setting. Real-world adherence rates are lower, contributing to the somewhat reduced outcomes observed in real-world observational studies compared to trial data.
Red Flags in “Dramatic” Before-and-After Content
Not all dramatic before-and-after content reflects straightforward Zepbound results. Several patterns should prompt skepticism:
Extremely rapid timelines. Transformation photos labeled “3 months” or “90 days” that show 30%+ body weight reduction are inconsistent with SURMOUNT-1 data. At 3 months on the dose-escalation ramp, most patients are at 5–10 mg range, where average 72-week outcomes are 15–19.5%, and the 3-month trajectory is considerably less. A photo showing bariatric-surgery-level results at 3 months on Zepbound almost certainly involves other interventions, very high starting weight, or non-standardized representation.
No dose or starting weight context. Percentage-based framing (“I lost 25% of my body weight!”) without context of starting weight and dose tells you very little. A patient starting at 400 lbs losing 25% (100 lbs) is not the same before-and-after as a patient starting at 200 lbs losing 25% (50 lbs), even though the percentages are identical.
Pre-existing or concurrent bariatric surgery. Some social media content combines GLP-1 medication use with prior or concurrent bariatric procedures. The results in such cases are not attributable to Zepbound alone and are not representative of the typical patient.
Promotional before-and-after images. Eli Lilly’s FDA-approved marketing for Zepbound is required to reflect realistic outcomes — but promotional content broadly, including affiliate content and telehealth provider advertising, is not always held to the same standard. Be cautious of images where lighting, posture, and clothing clearly maximize the visual contrast rather than accurately representing body composition.
Safety: What You Must Know Before Pursuing a Transformation
This is a YMYL article, and the safety section is not a formality.
FDA Contraindications and Black Box Warning
Zepbound carries a black box warning for the risk of thyroid C-cell tumors. Per the Zepbound prescribing information:
ZEPBOUND is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Counsel patients regarding the potential risk for MTC and inform them of symptoms including a mass in the neck, dysphagia, dyspnea, or persistent hoarseness.
Additional FDA-labeled contraindications include known serious hypersensitivity to tirzepatide or any excipient. Zepbound must not be combined with other tirzepatide-containing products (Mounjaro) or any other GLP-1 receptor agonist (semaglutide, liraglutide, dulaglutide, exenatide). See the FDA press release and full prescribing information for the complete contraindication list.
Serious Risks to Discuss With Your Provider
Beyond contraindications, important safety considerations per FDA labeling include: pancreatitis (discontinue if suspected); gallbladder disease (cholelithiasis and cholecystitis reported); acute kidney injury from GI-mediated fluid loss; hypoglycemia when combined with a sulfonylurea or insulin; worsening diabetic retinopathy in T2D patients; and aspiration risk under general anesthesia due to delayed gastric emptying. Inform all providers, including surgeons and anesthesiologists, that you are taking Zepbound before any procedure requiring sedation or general anesthesia.
Pregnancy
Zepbound may cause fetal harm. Discontinue Zepbound when pregnancy is recognized. A pregnancy exposure registry is available at 1-800-LillyRx. Patients on oral contraceptives should use backup or alternative contraception for 4 weeks after initiation and 4 weeks after each dose escalation, as delayed gastric emptying reduces oral medication absorption.
Realistic Expectations Are a Safety Issue
In the YMYL context, unrealistic expectations are not simply a matter of disappointment, they drive clinically unsafe behaviors. Patients who expect 30% loss in 3 months and see 8% may abandon a treatment that is working. Patients who see dramatic social media results may seek compounded tirzepatide from unregulated sources, which, as of April 2026, is not legal under standard 503A or 503B compounding, as both windows are closed per FDA clarification. Understanding what real results look like protects patients from both under-treatment and unsafe alternatives.
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: The before-and-after genre has a structural honesty problem. It selects for the most visually dramatic results, taken at the most favorable time point, from the most photogenic patients, using the highest doses after the longest treatment duration. Then it presents these as what Zepbound “does.” This is not wrong in a narrow technical sense, those are real results from real patients, but it is incomplete in a way that reliably misleads people who are trying to make medical decisions.
What SURMOUNT-1 actually shows is this: the average non-diabetic patient on 15 mg loses about 47 lbs from a 230-lb starting weight over 72 weeks. That is a clinically transformative result. It reduces waist circumference by nearly 8 inches, fasting insulin by 54%, and triglycerides by nearly 25%. It changes how someone moves through the world, how their joints feel, how their clothes fit, and what their labs look like. It is not equivalent to bariatric surgery at the population average, but for the 36% of 15 mg patients who lose 25% or more, the physical transformation is genuinely comparable to surgical outcomes in magnitude.
Patients deserve to see both the average and the distribution, not just the top of the distribution. At WeightLossInjections.com, we believe the average is compelling enough to speak for itself without the distortion of selective presentation.
To find out whether you are a candidate for Zepbound and begin treatment with a licensed provider, complete our free online eligibility assessment at WeightLossInjections.com. The bundled telehealth program is [$X/month] and includes [service detail].
Frequently Asked Questions
The published clinical average from SURMOUNT-1 in NEJM 2022 is 20.9% of body weight at 72 weeks on the 15 mg dose, among non-diabetic patients with obesity or overweight. For a person starting at 225 lbs, that is approximately 47 lbs. Lower doses produce lower averages: 15% at 5 mg and 19.5% at 10 mg. These are population averages with a distribution — some patients lose more, some lose less. Patients with type 2 diabetes average approximately 14.7% at 15 mg per SURMOUNT-2 in The Lancet 2023. There is no guarantee of any individual outcome; these are population-level means used for realistic expectation-setting.
Most patients begin noticing changes in the mirror and in clothing fit between months 2 and 4, after reaching and adapting to the 5–10 mg dose range. External social recognition (“you look different”) more commonly begins around months 4–6 for patients losing 14–18% of body weight. The most dramatic visual phase for most patients is months 4–9. The Zepbound prescribing information describes a minimum 20-week titration period to reach 15 mg, which means peak-dose effects are not fully established until approximately month 5.
Clinically, SURMOUNT-1 measured waist circumference reduction of −19.4 cm at 72 weeks, indicating significant visceral and abdominal fat loss. Patient-reported experience and community data consistently identify the face, neck, and abdominal region as the first areas where changes become visible. This is consistent with the metabolic pattern of GLP-1/GIP agonism, which preferentially reduces visceral adipose tissue.
Yes, most patients regain a significant portion of lost weight after stopping. SURMOUNT-4 in JAMA 2023 found that patients who stopped Zepbound after a 36-week lead-in period (during which they had lost an average 20.9%) regained 14.0% weight within 52 weeks, ending at only −9.9% from their original baseline. Only 16.6% of patients who stopped maintained ≥80% of their initial weight loss, compared to 89.5% of those who continued treatment. Obesity is a chronic condition, and Zepbound treats it chronically. Stopping medication typically restores the physiological drives toward weight regain.
Yes, reliably so. SURMOUNT-2 in The Lancet 2023 found average weight loss of 14.7% at 15 mg among T2D patients at 72 weeks, approximately 6 percentage points less than non-T2D patients in SURMOUNT-1. This is consistent with findings across GLP-1 and dual agonist medications: insulin resistance, T2D medications, and metabolic differences in T2D reduce the magnitude of weight loss. T2D patients do experience meaningful, clinically significant transformation on Zepbound; the results are simply calibrated differently. The added benefit for T2D patients is glycemic: HbA1c reduced by 2.08 percentage points at 15 mg, with 49% achieving normoglycemic levels per ACC SURMOUNT-2 summary.
In SURMOUNT-1 at the 15 mg dose, 57% of patients lost ≥20% of body weight at 72 weeks, more than half. At 10 mg, 49% reached that threshold; at 5 mg, 34%. At 25% body weight loss (the threshold most commonly associated with visually dramatic before-and-after photos), approximately 36% of 15 mg patients qualified. This means that roughly one in three patients on the highest dose achieves the level of transformation shown in the most dramatic before-and-after content.
This article is for educational purposes only and does not constitute medical advice. Zepbound (tirzepatide) is FDA-approved for chronic weight management (NDA 217806, November 8, 2023) and for moderate-to-severe obstructive sleep apnea in adults with obesity (December 20, 2024). Weight loss results vary; trial averages represent population means, not guaranteed outcomes for any individual. All clinical data cited reflects published peer-reviewed sources; verify current prescribing information with your provider. WeightLossInjections.com’s editorial team reviews all content quarterly; last medical review: April 2026. Consult a licensed healthcare provider before starting any prescription medication.
