![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/05/hero_zepbound_c5_lifestyle-1200x675.png)
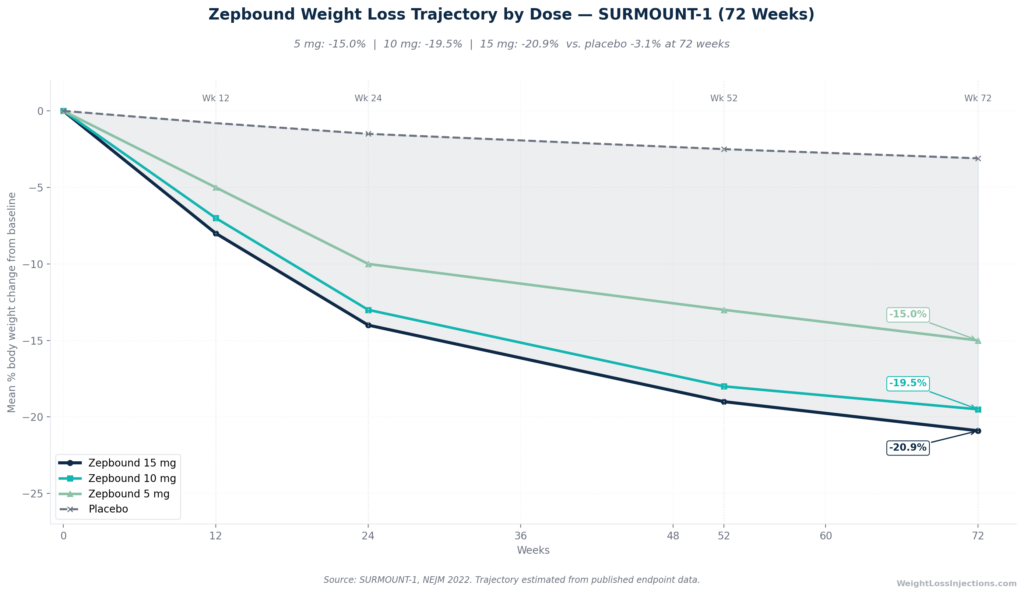
Zepbound Weight Loss Trajectory by Dose — SURMOUNT-1 (72 Weeks)
In the pivotal SURMOUNT-1 trial published in the New England Journal of Medicine, Zepbound produced mean weight reductions of −15.0% at 5 mg, −19.5% at 10 mg, and −20.9% at 15 mg at 72 weeks, compared to −3.1% on placebo. More than half of patients on the highest dose lost 20% or more of their body weight, a threshold historically associated with bariatric surgery. Results vary by dose reached, diabetes status, lifestyle integration, and time on treatment.
This guide walks through every stage of the Zepbound weight loss trajectory using primary clinical trial data.
How Zepbound Produces Weight Loss
Dual GIP/GLP-1 Mechanism
Zepbound (tirzepatide) is the first approved dual agonist of the glucose-dependent insulinotropic polypeptide receptor (GIPR) and the GLP-1 receptor (GLP-1R). Per the Zepbound FDA prescribing information, it activates both incretin pathways simultaneously, driving appetite suppression through hypothalamic satiety centers, slowing gastric emptying, and reducing adipogenesis through direct effects on adipose tissue GIPR. The added GIP component distinguishes tirzepatide from GLP-1-only agents such as semaglutide: the dual mechanism deepens appetite suppression and improves metabolic markers beyond what single-pathway agonists achieve.
The practical result is a sustained, progressive reduction in caloric intake that does not feel like restriction to most patients. Hunger quiets. Portions shrink naturally. Cravings, particularly for calorie-dense foods, diminish. These effects strengthen as the dose escalates.
The Titration Phase: Why Your First Weeks Look Modest
Per the Zepbound prescribing information, the starting dose of 2.5 mg is explicitly a tolerability step, it is not an approved maintenance dose, and it is not designed to produce peak weight loss. The full titration sequence, 2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg, each step requiring at least four weeks, means that reaching the maximum dose takes a minimum of 20 weeks from day one, per the FDA approval announcement from November 8, 2023. Every dose increase also restarts a brief GI adaptation window. Patients who evaluate results during the first four weeks at 2.5 mg are judging the tolerance phase, not the treatment phase.
The weight loss curve is not linear: it accelerates as you ascend the dose ladder, peaks around weeks 32–52, then flattens toward a plateau near 72 weeks, which is where SURMOUNT-1 ended.
What the Trials Actually Showed: The Full SURMOUNT Program
No competitor article presents the complete SURMOUNT program in one place. Here is that picture, drawn from primary publications.
SURMOUNT-1: Non-Diabetic Obesity at 72 Weeks
SURMOUNT-1, published in the New England Journal of Medicine in 2022 by Jastreboff et al., is the foundational efficacy study. Design: 2,539 adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one comorbidity, without type 2 diabetes; 72-week primary treatment period; randomized to tirzepatide 5 mg, 10 mg, 15 mg, or placebo.
Weight loss at 72 weeks (treatment-regimen estimand):
| Dose | Mean % Weight Loss | vs. Placebo |
|---|---|---|
| 5 mg | −15.0% | −11.9 pp |
| 10 mg | −19.5% | −16.4 pp |
| 15 mg | −20.9% | −17.8 pp |
| Placebo | −3.1% | — |
Source: SURMOUNT-1, NEJM 2022; Lilly press release, June 4, 2022.
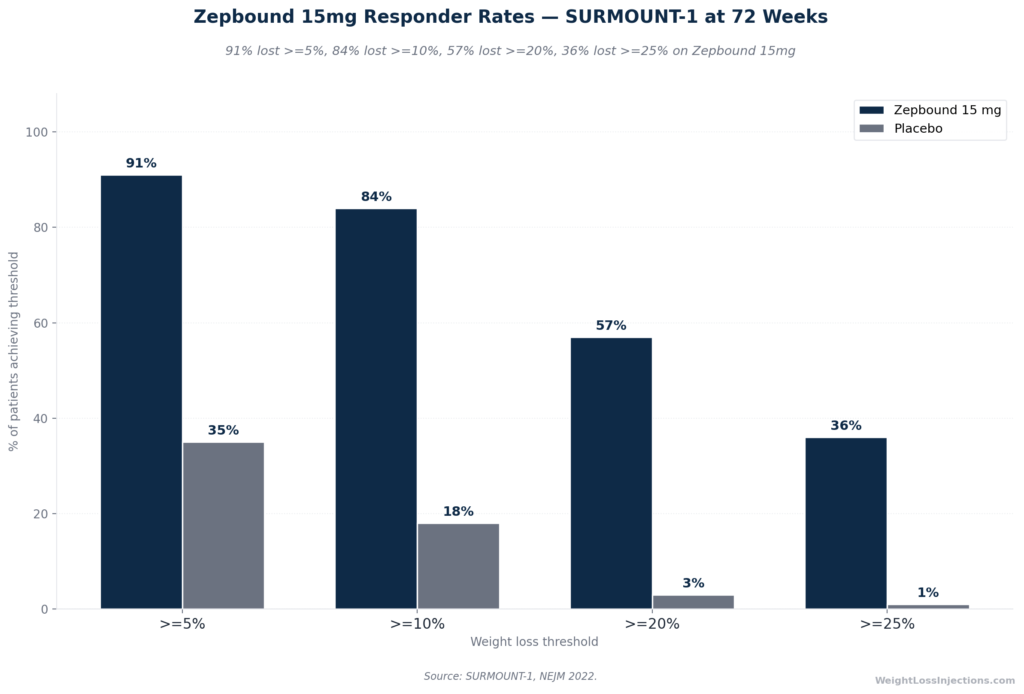
Responder rates at 15 mg:
- ≥5% body weight loss: 91% vs. 35% placebo
- ≥10% body weight loss: 84% vs. 18% placebo
- ≥20% body weight loss: 57% vs. 3% placebo
- ≥25% body weight loss: 36%
The 57% figure deserves to sit with you for a moment. More than half of patients on the maximum dose lost at least one-fifth of their starting body weight, a result the American College of Cardiology’s SURMOUNT-1 trial summary notes was historically associated only with bariatric surgery.
Zepbound 15 mg Responder Rates — SURMOUNT-1 at 72 Weeks
SURMOUNT-2: Obesity With Type 2 Diabetes at 72 Weeks
SURMOUNT-2, published in The Lancet in 2023, enrolled 938 adults with BMI ≥27 and established type 2 diabetes (HbA1c 7–10%) for a 72-week trial at tirzepatide 10 mg and 15 mg versus placebo. Weight loss at the maximum dose reached −14.7% (10 mg: −12.8%), versus −3.2% placebo, approximately 6 percentage points less than in the non-diabetic SURMOUNT-1 cohort, per the ACC SURMOUNT-2 trial summary. The glycemic benefit was substantial: HbA1c fell by −2.08% at 15 mg, and 49% of tirzepatide patients achieved normoglycemic HbA1c below 5.7%, a level rarely achieved with any pharmacotherapy in a T2D population.
The critical takeaway: diabetes status meaningfully reduces weight loss on Zepbound, but 14.7% at 72 weeks still represents clinically significant loss in a metabolically complex population.
SURMOUNT-3: What Happens When You Combine Drug With Intensive Lifestyle
SURMOUNT-3, published in Nature Medicine in 2023, added a structural twist: a 12-week intensive lifestyle intervention lead-in before randomization. Only participants who achieved ≥5% weight loss during the lead-in proceeded. From randomization, tirzepatide added a further −18.4% versus +2.5% for placebo. Total weight loss from study entry was −24.3% for the tirzepatide group, approximating outcomes seen after sleeve gastrectomy at one year.
Important limitation for interpretation: the −24.3% total includes the lead-in lifestyle phase. The drug’s contribution from randomization was −18.4%. SURMOUNT-3 shows that structured lifestyle adds roughly 4–6 percentage points over standard counseling, but it does not mean every patient who takes Zepbound will lose 24%. The study design selected for patients already responding to lifestyle intervention.
SURMOUNT-4: The Withdrawal Study and What It Reveals About Long-Term Treatment
SURMOUNT-4, published in JAMA in 2023, is the most practically important trial for patients considering how long to stay on Zepbound. Design: 783 patients, 36-week open-label tirzepatide lead-in, then randomized 1:1 to continue tirzepatide or switch to placebo for 52 more weeks.
Results from the SURMOUNT-4 PubMed abstract:
- At the end of the lead-in (week 36): mean −20.9% weight loss
- Weeks 36–88 on continued tirzepatide: additional −5.5%
- Weeks 36–88 on placebo (withdrawal): +14.0% regain
- Overall week 0–88 loss: −25.3% (continuation) vs. −9.9% (withdrawal)
- 89.5% of continuation patients maintained ≥80% of their lead-in loss; only 16.6% of withdrawal patients did so
The message is unambiguous: stopping Zepbound leads to substantial weight regain. Obesity is a chronic disease, not a condition that self-resolves after a course of treatment. Patients who plan to use Zepbound as a fixed-duration treatment should understand this data before starting.
3-Year Extension: Durability in a Prediabetes Subgroup
A prediabetes subgroup from SURMOUNT-1 was followed for 176 weeks (approximately 3.4 years). Per the NEJM 2025 extension paper by Jastreboff et al., mean weight reduction remained at −19.7% (15 mg) versus −1.3% placebo at 176 weeks, and progression to type 2 diabetes was reduced by 88% (2.4% tirzepatide vs. 13.7% placebo after a 17-week off-treatment washout period). Note: this data comes from a prediabetes subgroup, not the full SURMOUNT-1 population. Results may not be representative of all Zepbound users.
Complete SURMOUNT Program Summary
| Trial | Population | Duration | Tirzepatide Dose | Mean % Weight Loss | Placebo |
|---|---|---|---|---|---|
| SURMOUNT-1 | Non-T2D obesity | 72 weeks | 15 mg | −20.9% | −3.1% |
| SURMOUNT-1 | Non-T2D obesity | 72 weeks | 10 mg | −19.5% | −3.1% |
| SURMOUNT-1 | Non-T2D obesity | 72 weeks | 5 mg | −15.0% | −3.1% |
| SURMOUNT-2 | Obesity + T2D | 72 weeks | 15 mg | −14.7% | −3.2% |
| SURMOUNT-2 | Obesity + T2D | 72 weeks | 10 mg | −12.8% | −3.2% |
| SURMOUNT-3 | Non-T2D (post-lifestyle lead-in) | 72 wk + 12 wk lead-in | MTD 10–15 mg | −24.3% (from entry) | −4.5% |
| SURMOUNT-4 | Non-T2D obesity (continued) | 88 weeks | MTD 10–15 mg | −25.3% | −9.9% (withdrawal) |
| SURMOUNT-1 extension | Prediabetes subgroup | 176 weeks | 15 mg | −19.7% | −1.3% |
Sources: SURMOUNT-1 NEJM 2022; SURMOUNT-2 Lancet 2023; SURMOUNT-3 Nature Medicine 2023; SURMOUNT-4 JAMA 2023; SURMOUNT-1 extension NEJM 2025.
Month-by-Month Weight Loss Timeline
This section draws on the SURMOUNT-1 treatment-regimen estimand and the titration schedule embedded in the Zepbound prescribing information to construct the most granular monthly picture the primary evidence supports. Individual results vary; these are trial-derived averages, not guarantees.
Month 1 (Weeks 1–4): The Tolerance Phase
You are at 2.5 mg — a dose the prescribing information classifies as a tolerability step, not a maintenance dose. Weight loss during this period is modest by design. Appetite suppression is beginning, but the drug has not yet reached the concentrations that drive meaningful caloric restriction. Expect GI symptoms (nausea, constipation) to be at their most prominent during weeks 1–3 as your system adapts.
Realistic month 1 estimate: ~1–3% body weight loss for most patients. For a person starting at 220 lbs, that is roughly 2–7 lbs — primarily reflecting reduced food intake and possible fluid shifts, not sustained fat loss.
What you may notice: smaller appetite at meals, earlier satiety, reduced interest in snacking. These are signs the mechanism is working, even if the scale is not yet dramatic.
Month 3 (Around Week 12): Entering the Active Loss Window
By week 12, most patients following standard titration are at or approaching 7.5–10 mg. SURMOUNT-1 data shows approximately 7–10% cumulative weight loss in the 10–15 mg arms by this milestone, per SURMOUNT-1 in NEJM. Shared Spec clinical guidance aligns with ~3–5% for those still in early titration, and up to 10% for patients who have escalated to 10 mg by this point.
Realistic month 3 benchmark: ~5–10% cumulative, dose-dependent. For a 220-lb starting weight, that is 11–22 lbs. Clothes fit differently. Blood pressure and fasting glucose typically begin improving.
This is the window where most patients first report the experience of “this is actually working.” Loss is visually noticeable.
Month 6 (Around Week 24): Peak Rate of Loss
Weeks 20–32 represent the steepest portion of the Zepbound weight loss curve for most patients. Many have reached 10–15 mg maintenance doses. SURMOUNT-1 data at 24 weeks shows approximately 14–16% cumulative loss in the 15 mg arm, consistent with the ~10–12% benchmark in the Shared Spec for the full titrating population (NEJM 2022).
Realistic month 6 benchmark: ~12–16% cumulative at 15 mg; somewhat less at 10 mg. For a 220-lb patient at 15 mg, that is approximately 26–35 lbs lost. Most dramatic changes in body shape, energy, and metabolic labs occur during this phase.
Month 12 (Around Week 52): Approaching the Plateau
Weight loss rate slows markedly after week 36–40 as the body begins defending its new lower weight. By week 52, SURMOUNT-1 patients at 15 mg had achieved approximately 18–20% cumulative loss, with most of the loss already accomplished by month 6 (NEJM 2022). The rate of change drops from perhaps 1–2 lbs per week at peak to fractions of a pound per week by month 12.
Realistic month 12 benchmark: ~18–21% at 15 mg; ~17–19% at 10 mg. For a 220-lb patient at 15 mg, approximately 40–46 lbs from starting weight.
This plateau is not treatment failure. It reflects a new metabolic equilibrium — the body is now maintaining a substantially lower weight with the drug’s support.
Week 72: The Trial Endpoint and What Comes Next
At 72 weeks, SURMOUNT-1 primary endpoints were reached: −20.9% (15 mg), −19.5% (10 mg), −15.0% (5 mg) versus −3.1% placebo (NEJM 2022). From week 52 to week 72, the marginal change was small — the plateau had set in. Most of the lifetime weight loss on Zepbound is captured by month 12–15.
What happens after week 72 on continued treatment: SURMOUNT-4 continuation data shows a further −5.5% reduction beyond the 36-week plateau, suggesting the body continues to slowly adapt even past the trial endpoint (SURMOUNT-4, JAMA 2023). The 3-year extension data shows durability at −19.7% for the prediabetes subgroup at 176 weeks (NEJM 2025).
Summary Table: Weight Loss by Phase
| Timeframe | Dose Range | Avg. Cumulative Loss | What to Expect |
|---|---|---|---|
| Weeks 1–4 (Month 1) | 2.5 mg | ~1–3% | Appetite starts quieting; GI adaptation; modest scale change |
| Weeks 5–8 | 5 mg | ~3–5% | Appetite noticeably reduced; first clear scale movement |
| Weeks 9–12 | 7.5–10 mg | ~7–10% | Clothes fitting differently; energy improving |
| Months 4–6 | 10–15 mg | ~12–16% | Most dramatic visual changes; peak rate of loss |
| Months 7–12 | 15 mg | ~18–21% | Loss slows as body adapts to new weight |
| 12–18 months | 15 mg maintenance | Up to ~21% (SURMOUNT-1 avg) | Plateau; metabolic markers continuing to improve |
*Data derived from SURMOUNT-1 treatment-regimen estimand. SURMOUNT-1, *NEJM* 2022.*
15 mg vs. 10 mg vs. 5 mg: What the Dose-Response Data Shows
The dose-response relationship in SURMOUNT-1 is consistent and clinically meaningful — a higher dose produces more weight loss, and the difference between doses is not trivial.
At 72 weeks, the gap between 5 mg and 15 mg is 5.9 percentage points (15.0% vs. 20.9%). For a 220-lb patient, that translates to approximately 13 additional pounds of weight loss over the course of treatment by reaching the maximum dose rather than staying at the minimum maintenance dose.
The responder analysis sharpens this picture. At 15 mg, 57% of patients lost ≥20% of body weight versus 32% at 5 mg and 45% at 10 mg (SURMOUNT-1, NEJM 2022). The ≥25% threshold — which approximates surgical outcomes — was achieved by 36% at 15 mg.
Practical implication: Patients who are tolerating lower doses well have a strong evidence-based rationale for continuing to escalate toward the maximum dose rather than staying at a comfortable lower level. The FDA-approved titration schedule allows escalation every four weeks minimum, and the incremental efficacy data from SURMOUNT-1 supports doing so when tolerated. For more on dose escalation decisions, see our guide at WeightLossInjections.com/why-increase-zepbound-dose/.
Beyond the Scale: Metabolic Marker Changes
Weight is one outcome. SURMOUNT-1 measured several others at 72 weeks on tirzepatide 15 mg that competitors’ articles consistently omit (NEJM 2022):
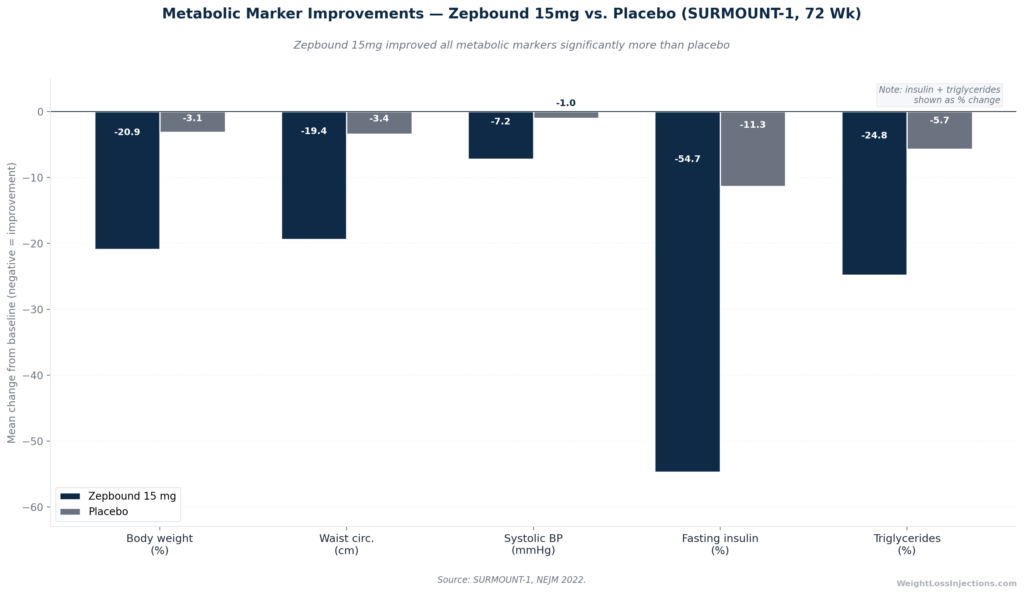
Metabolic Marker Improvements — Zepbound 15 mg vs. Placebo, SURMOUNT-1 72 Weeks
| Metabolic Marker | Zepbound 15 mg | Placebo |
|---|---|---|
| Body weight | −20.9% | −3.1% |
| Waist circumference | −19.4 cm (~7.6 inches) | −3.4 cm |
| BMI | −7.7 points | −1.1 points |
| Systolic blood pressure | −7.2 mmHg | −1.0 mmHg |
| Fasting insulin | −54.7% | −11.3% |
| Triglycerides | −24.8% | −5.7% |
Source: SURMOUNT-1, NEJM 2022.
The fasting insulin reduction of 54.7% is particularly striking — it reflects a meaningful shift in insulin resistance, not merely the downstream effect of weighing less. Cardiovascular risk reduction through improved blood pressure and triglycerides occurs in parallel with weight change, and these improvements compound over time.
Factors That Predict Higher or Lower Weight Loss
No two patients experience the same Zepbound results. These are the primary variables the clinical evidence identifies.
1. Dose Reached and Maintained
This is the single strongest predictor within a patient’s control. The dose-response data from SURMOUNT-1 is unambiguous: every dose step up adds efficacy. Patients who reach and sustain 15 mg consistently outperform those who remain at 5 mg (NEJM 2022). If GI side effects are the reason for staying at a lower dose, discuss management strategies with your provider — dose reduction or slower titration is a legitimate option that preserves long-term progress.
2. Type 2 Diabetes Status
T2D patients lose approximately 6 percentage points less than non-diabetic patients at equivalent doses: 14.7% at 15 mg (SURMOUNT-2) versus 20.9% (SURMOUNT-1), per the ACC SURMOUNT-2 trial summary. The mechanisms include insulin resistance impairing lipolysis, co-occurring medications that promote weight gain, and potentially blunted receptor-level effects in the diabetic metabolic environment. T2D patients still achieve substantial, clinically meaningful weight loss — but should calibrate expectations to SURMOUNT-2 figures, not SURMOUNT-1.
3. Lifestyle Integration
SURMOUNT-3 provides the clearest data on this: adding structured, intensive lifestyle intervention to tirzepatide produces total loss of −24.3% from study entry, versus the standard −20.9% in SURMOUNT-1 (Nature Medicine 2023). The drug does the heavy lifting, but diet quality, protein adequacy, and physical activity all contribute meaningfully — especially for preserving lean mass and maintaining losses long-term.
4. Starting BMI and Body Weight
Patients with higher starting BMI tend to lose more absolute weight in pounds, while percentage loss is broadly consistent across BMI groups. A patient starting at 300 lbs losing 20% sheds 60 lbs; a patient at 200 lbs losing 20% sheds 40 lbs. Both are substantial. Percentage is the more clinically meaningful comparator because it reflects the metabolic burden of excess weight.
5. Sex and Hormonal Factors
SURMOUNT-1 subgroup analyses suggest modest differences by sex, with female patients tending to lose slightly more percentage weight than male patients at equivalent doses, consistent with patterns seen across GLP-1 and GIP/GLP-1 agents. This effect is smaller than the dose or diabetes-status effect and should not be over-interpreted.
6. Adherence and Injection Consistency
Steady-state plasma concentration for tirzepatide is achieved after approximately four weeks of once-weekly dosing at each dose level, per the Zepbound prescribing information. Missing doses breaks that steady-state, reducing plasma drug levels and blunting appetite suppression. Consistent weekly injection timing, not just dose, is a meaningful predictor of outcome. If a dose is missed and fewer than four days (96 hours) have elapsed, take it as soon as possible. If more than four days have passed, skip and resume the regular schedule.
7. Prior Weight Loss History and Set-Point Biology
Patients with a history of repeated cycles of weight loss and regain (“yo-yo dieting”) may have altered adipokine signaling and reduced metabolic flexibility. While tirzepatide’s dual mechanism appears to work effectively even in patients with prior weight loss attempts, a body that has been defended at a higher weight for many years may require more time to adapt. This is a biological reality, not a character flaw.
Our Top 3 · July 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
The 72-Week Plateau: What It Means and What to Do
By weeks 60–72 of SURMOUNT-1, the weight loss curve had largely flattened, mean change in the 15 mg arm moved from approximately −19% at week 52 to −20.9% at week 72 (NEJM 2022). This plateau reflects the body achieving a new homeostatic equilibrium at a lower weight, with Zepbound now working to maintain that weight rather than drive further loss.
Two distinct plateau scenarios require different responses:
Titration-phase plateau (before reaching maintenance dose): If weight loss has stalled while you are still on 2.5 mg, 5 mg, or 7.5 mg, the appropriate clinical question is dose escalation. Sub-maintenance doses are not the destination. Per the Zepbound dosing page at Zepbound.lilly.com, approved maintenance doses are 5 mg, 10 mg, and 15 mg — patients on lower doses who are tolerating treatment should discuss escalation with their provider. See our full guide on when to increase your Zepbound dose at WeightLossInjections.com/why-increase-zepbound-dose/.
True maintenance-dose plateau (at 10 mg or 15 mg after 52+ weeks): This is expected and represents treatment success, not failure. The goal at this phase shifts from loss to preservation. Lifestyle factors become more important as the drug-driven caloric deficit stabilizes. Some patients work with providers to assess whether a modest dose reduction is appropriate once a significant stable weight loss has been achieved, though current SURMOUNT-4 data suggests continued treatment at the original dose best preserves results.
What is not a plateau: A two-to-four week period of no scale movement while titrating doses is a normal interlude as the body adapts to the new dose. Day-to-day weight fluctuations of 2–5 lbs from water, sodium, and hormonal cycles are not meaningful. Track a weekly average, not daily readings.
What Happens After Discontinuation: SURMOUNT-4 Regain Data
The SURMOUNT-4 withdrawal arm is the most important data set for patients considering stopping Zepbound after reaching their goal weight. After the 36-week lead-in (mean −20.9% loss), patients who switched to placebo regained 14.0% of body weight over the following 52 weeks, ending at a net −9.9% from baseline, meaning they retained less than half of their original loss (SURMOUNT-4 JAMA 2023; PubMed abstract).
By contrast, patients who continued tirzepatide lost a further 5.5%, reaching −25.3% overall, and 89.5% of continuation patients maintained ≥80% of their lead-in loss at week 88 (JAMA 2023).
Obesity is a chronic, neurobiologically mediated disease. Zepbound suppresses appetite signaling continuously; when the drug stops, those signals return. The regain in SURMOUNT-4 was not due to behavioral failure, it occurred uniformly across the withdrawal group. Most providers prescribing Zepbound discuss this data with patients and plan for indefinite treatment unless a medical contraindication develops.
Realistic Week-by-Week Expectations: Slow vs. Fast Responders
“Fast” Responders
Roughly 20–25% of Zepbound patients lose weight at the upper end of the distribution, approaching or exceeding the trial averages from the early stages of titration. Characteristics common among faster responders include: non-diabetic metabolic status, higher starting BMI providing more room for absolute loss, early high adherence to dietary changes, and physiologic GIP/GLP-1 receptor sensitivity. Fast responders are likely to reach the ≥20% threshold at 72 weeks — recall that 57% of 15 mg patients hit this mark in SURMOUNT-1 (NEJM 2022), which means fast response is actually the majority experience at full dose.
“Slow” Responders
Slow response — less than 5% loss after 12 weeks at 5 mg or higher — warrants a clinical review. Possible contributing factors:
- Diabetes status: Reduces expected loss by ~6 pp; slower loss is the expected norm in T2D patients, not non-response
- Medications that promote weight gain: Corticosteroids, certain antidepressants (mirtazapine, some SSRIs), insulin, and antipsychotics can counteract GLP-1 mechanism
- Thyroid dysfunction: Undiagnosed or undertreated hypothyroidism significantly impairs weight loss response and should be evaluated before labeling any patient a non-responder
- Sleep deprivation: Chronic sleep insufficiency elevates ghrelin and cortisol, partially counteracting appetite suppression
- Caloric compensation: Some patients unconsciously compensate for reduced hunger by consuming more calorie-dense foods, undermining the drug’s caloric-restriction effect
True pharmacological non-response to tirzepatide at adequate doses is uncommon given the drug’s dual mechanism and the consistent efficacy seen across SURMOUNT-1’s population. If loss has genuinely plateaued below 5% at 5 mg or higher, a structured clinical assessment, not abandonment of treatment, is the appropriate next step.
Body Composition: Fat Loss vs. Muscle Mass
A consistent finding across GLP-1 and dual GIP/GLP-1 agents: a portion of total weight lost is lean mass, not just fat. SURMOUNT-1 data from DXA substudies (dual-energy X-ray absorptiometry) confirmed that while most weight loss was from fat mass, lean mass also declined, a pattern common to any caloric-deficit-driven weight loss, including diet alone.
The implications matter for metabolic health and long-term maintenance:
1. Preserve lean mass with protein intake: During rapid weight loss, adequate dietary protein (approximately 1.2–1.6 g per kilogram of body weight per day, per standard obesity medicine clinical guidance) attenuates muscle catabolism. Lean meats, fish, eggs, Greek yogurt, and legumes provide protein without the high caloric density that undermines the drug’s effect.
2. Resistance training protects muscle: Two to three sessions per week of compound strength movements (squats, rows, presses) during active weight loss preserves metabolic muscle. Muscle is metabolically active tissue; preserving it maintains resting energy expenditure and reduces the risk of weight regain if treatment is discontinued or doses are reduced.
3. The fat-loss signal is the meaningful one: The waist circumference reduction of −19.4 cm in SURMOUNT-1 at 15 mg (NEJM 2022) reflects visceral and subcutaneous fat loss, the component most directly linked to cardiovascular and metabolic risk. The absolute proportion of fat vs. lean mass in total weight loss on tirzepatide compares favorably to diet-only or prior-generation pharmacotherapy.
What “Slow Weight Loss” Really Means, and When to Act
If your weight loss on Zepbound feels slower than expected, the first question is: slower than what, exactly? The SURMOUNT-1 averages are population means, they describe the middle of the distribution, not a minimum standard.
Consider the following before concluding treatment isn’t working:
| Scenario | What’s Actually Happening | Recommended Action |
|---|---|---|
| No loss at 2.5 mg in weeks 1–4 | Expected — this is the tolerance dose | Continue to 5 mg per schedule |
| <5% loss at 4 months (still titrating) | Dose may not be optimized yet | Discuss escalation with provider |
| <5% loss at 5 mg for 8+ weeks | Possible non-response or confounders | Provider review: T2D, medications, thyroid, adherence |
| 10–15% loss plateau at 12 months | Normal trial-pattern plateau | Expected; focus on maintenance and lifestyle |
| Weight regain after reaching goal | Consistent with SURMOUNT-4 biology | Discuss long-term treatment plan before reducing dose |
The single biggest error patients make is interpreting the titration plateau (stalled loss while dose is still being escalated) as evidence the drug doesn’t work for them. The dose isn’t there yet.
Practical Logging Tools for Tracking Your Results
Systematic self-monitoring during Zepbound treatment improves awareness of progress beyond the scale and helps identify patterns that affect outcomes:
Weekly weigh-ins (same time, same conditions): Weigh first thing in the morning, after using the bathroom, before eating or drinking, and wearing the same clothing (or none). Day-to-day fluctuations of 2–5 lbs from sodium, hydration, and hormonal cycles are normal noise. A weekly average trend is the signal. Apps such as Happy Scale or Libra smooth out daily variability with a moving average.
Waist circumference: Measure at the level of the navel (or just above the iliac crest per standard protocol) weekly. SURMOUNT-1 showed −19.4 cm at 72 weeks, tracking this metric captures visceral fat loss that sometimes precedes changes on the scale (NEJM 2022).
Injection log: Note dose, injection site, injection date, and any side effects. Rotating injection sites (abdomen, outer thigh, or upper arm per Zepbound Instructions for Use) reduces local tissue reaction and ensures consistent absorption.
Dietary protein log: During active loss, tracking protein intake for even two to four weeks helps calibrate whether you are consuming enough to protect lean mass. Free apps (Cronometer, MyFitnessPal) make this straightforward.
Labs at baseline, 3 months, and 6 months: Fasting glucose, HbA1c (if diabetic), fasting lipid panel, and TSH (to rule out thyroid dysfunction as a confounder) give a comprehensive view of metabolic progress beyond the scale.
Our take at WeightLossInjections.com: The SURMOUNT-1 data is genuinely remarkable, but the patients who achieve the best outcomes are not passive recipients of those statistics. They escalate to the maximum tolerated dose, maintain consistent weekly injections, use the drug’s appetite-suppression signal to support better dietary choices, protect their lean mass with protein and strength training, and go in with realistic, phase-appropriate expectations. Month 1 on 2.5 mg is the price of admission. Month 12 on 15 mg, for most patients who get there, looks like a different body entirely. The key is understanding the curve well enough to stay on it when the scale moves slowly.
Frequently Asked Questions
At three months (approximately week 12), most patients following standard titration are approaching 7.5–10 mg and have experienced roughly 5–10% cumulative weight loss, based on SURMOUNT-1 trajectory data. The exact figure depends heavily on where you are in the titration schedule. Patients who are still at 5 mg at week 12 are likely closer to 5%; patients who have escalated to 10 mg may approach 10%. For a person starting at 200 lbs, 5–10% translates to approximately 10–20 lbs in the first three months.
The first question is: which dose are you on? At 2.5 mg (weeks 1–4), minimal loss is expected, this is a tolerability dose, not a maintenance dose per the Zepbound prescribing information. At 5 mg or higher with no movement after 8–12 weeks, a clinical review is warranted. Key factors to evaluate: adherence and injection technique, type 2 diabetes status (which reduces expected loss by ~6 percentage points per SURMOUNT-2), thyroid function, any medications that promote weight gain (corticosteroids, certain antidepressants, insulin), sleep quality, and caloric intake. True pharmacological non-response at therapeutic doses is uncommon but exists, and deserves a proper evaluation, not abandonment of treatment.
No. In SURMOUNT-1, 57% of patients on the maximum 15 mg dose lost ≥20% of body weight at 72 weeks (NEJM 2022), meaning 43% did not reach that threshold even at the highest dose. At 10 mg, 45% reached ≥20%; at 5 mg, 32%. Reaching 15 mg and maintaining it for 72 weeks is itself an accomplishment not all patients achieve. The trial average of −20.9% at 15 mg is a mean across the distribution; individual results range considerably. Clinically meaningful weight loss of 5–10%, achievable by the large majority of patients at any approved maintenance dose — carries substantial cardiovascular and metabolic benefit regardless of whether it reaches the 20% surgical threshold.
SURMOUNT-4 published in JAMA 2023 answers this directly: patients who discontinued tirzepatide after achieving −20.9% loss during the 36-week lead-in regained an average of 14.0% of body weight over the following 52 weeks, ending at just −9.9% from their original starting weight. Only 16.6% of withdrawal patients maintained ≥80% of their lost weight, compared to 89.5% on continued treatment. Stopping Zepbound does not “lock in” results, obesity is a chronic disease with a biological drive toward weight regain when treatment is removed.
Head-to-head trial data comparing tirzepatide (Zepbound) to semaglutide 2.4 mg (Wegovy) at equivalent doses is available from the SURMOUNT-5 trial, which showed tirzepatide achieved greater weight loss. Indirect comparison from separate trials: Zepbound at 15 mg produced −20.9% at 72 weeks (SURMOUNT-1, NEJM 2022); Wegovy at 2.4 mg produced −14.9% at 68 weeks in the STEP 1 trial. The dual GIP/GLP-1 mechanism appears to drive deeper weight loss than GLP-1-only agents. See our full comparison at WeightLossInjections.com/zepbound-vs-wegovy/.
No, it works in T2D patients, but it works less for weight loss specifically. T2D patients lose approximately 6 percentage points less than non-diabetic patients at equivalent doses: −14.7% vs. −20.9% at 15 mg in SURMOUNT-2 versus SURMOUNT-1, per the ACC SURMOUNT-2 summary. The glycemic benefits are also substantial, HbA1c fell by −2.08% at 15 mg in SURMOUNT-2, with 49% of tirzepatide patients achieving normoglycemic levels. T2D patients should calibrate weight loss expectations to SURMOUNT-2 figures, not SURMOUNT-1, 14.7% at 72 weeks is still clinically meaningful, but it is not the 20.9% that non-diabetic trial averages suggest.
This article is for educational purposes only and does not constitute medical advice. Zepbound is FDA-approved for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity, and for moderate-to-severe obstructive sleep apnea in adults with obesity. Weight loss results vary by individual; clinical trial averages represent population means and do not guarantee any specific outcome. WeightLossInjections.com’s editorial team reviews all content quarterly; last medical review: April 2026. Consult a licensed provider before starting any prescription medication.
