![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/05/hero_zepbound_c4_compare-1200x675.png)
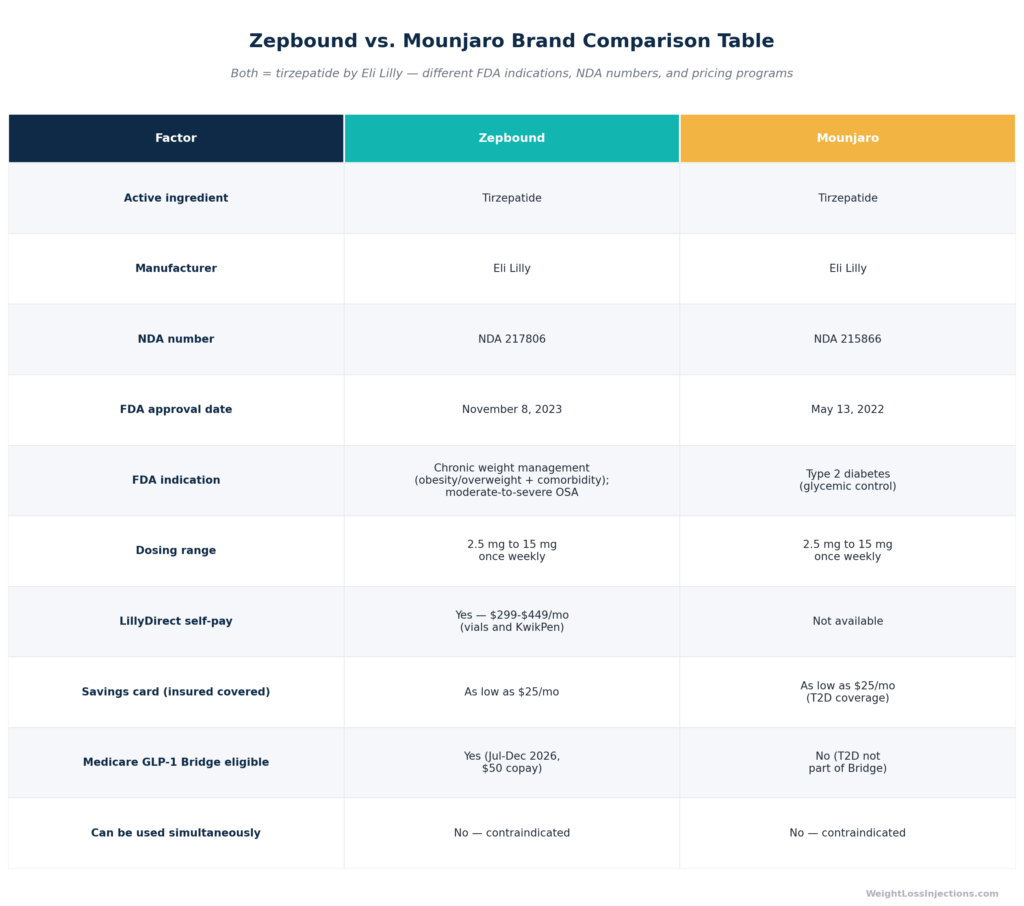
Zepbound vs. Mounjaro Brand Comparison Table
Zepbound and Mounjaro contain the exact same molecule, tirzepatide, manufactured by Eli Lilly to the same specifications. The critical difference is FDA indication: Mounjaro (NDA 215866) is approved for type 2 diabetes; Zepbound (NDA 217806) is approved for chronic weight management and obstructive sleep apnea.
That single regulatory distinction determines your insurance coverage pathway, your savings card, and whether you can access LillyDirect’s $299–$449/mo self-pay pricing. You cannot substitute one at the pharmacy counter, they require separate prescriptions, and they must never be used together.
The Short Answer: Same Molecule, Different Label
If a colleague told you Zepbound and Mounjaro are the same drug, they are correct at the chemical level and wrong at the regulatory level. Both products contain tirzepatide, a synthetic 39-amino acid peptide with the molecular formula C₂₂₅H₃₄₈N₄₈O₆₈ and an elimination half-life of approximately 5–6 days, manufactured at the same Eli Lilly facilities to identical specifications, per the Zepbound prescribing information. Same active ingredient. Same concentration per 0.5 mL injection. Same titration schedule.
What differs is everything that sits on top of the molecule: the FDA indication, the NDA number, the insurance billing codes, the savings programs, and in 2026, who has access to LillyDirect’s direct-to-consumer pricing. For a patient deciding which brand to ask for, those differences are consequential enough to change both the cost and the coverage outcome by thousands of dollars per year.
This article explains each difference clearly, works through who should ask for which brand, and covers the one question competitors consistently skip: how the insurance coding difference between Mounjaro (diabetes ICD-10 codes) and Zepbound (obesity ICD-10 codes) affects your prior authorization pathway and your options if coverage is denied.
Why Does Eli Lilly Have Two Brands for One Drug?
The two-brand structure is not a marketing gimmick. It reflects how the FDA drug approval system works.
FDA approval is indication-specific. A manufacturer must file a separate New Drug Application for each approved use of an active ingredient, supported by independent clinical trial data for that indication. Eli Lilly ran two parallel development programs for tirzepatide: the SURPASS program (type 2 diabetes) and the SURMOUNT program (obesity and overweight). Each program required its own phase 3 evidence, its own regulatory submission, and its own NDA review.
NDA 215866 was approved May 13, 2022, based on the SURPASS data for glycemic control in adults with T2D. That product became Mounjaro. NDA 217806 was approved November 8, 2023, based on the SURMOUNT data for chronic weight management. That product became Zepbound. A third approval followed on December 20, 2024, when the FDA approved Zepbound as the first and only prescription medicine for moderate-to-severe obstructive sleep apnea in adults with obesity, a second indication for the Zepbound NDA, not a third brand.
The practical consequence: the brand name tells your insurer which indication you are being treated for, which determines the ICD-10 diagnosis code on your prior authorization, which determines whether your diabetes benefit or your obesity benefit applies. This is not cosmetic. It is the billing framework that governs coverage.
FDA Indications: A Side-by-Side Comparison
Mounjaro: Type 2 Diabetes Only
Mounjaro’s FDA label is narrow: it is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. That is the entirety of Mounjaro’s on-label indication. Mounjaro has no weight management indication and no OSA indication, per Drugs@FDA NDA 215866.
This matters in one important way: many providers have prescribed Mounjaro off-label for weight loss in patients who do not have T2D. Clinically, the drug works identically. Legally and financially, it creates a coverage problem. Off-label Mounjaro for weight loss will not be billed under T2D codes (the patient does not have T2D), and insurers will not reimburse it under obesity codes (Mounjaro has no obesity indication). The patient typically pays list price or out-of-pocket.
Zepbound: Weight Management and OSA
Zepbound’s label covers two FDA-approved indications:
- Chronic weight management: As an adjunct to a reduced-calorie diet and increased physical activity for adults with obesity (BMI ≥30 kg/m²) or overweight (BMI ≥27 kg/m²) with at least one weight-related comorbid condition — such as hypertension, type 2 diabetes, or dyslipidemia — per the FDA Zepbound approval press release. Note that T2D is listed as a qualifying comorbidity for the weight management indication — meaning a patient with T2D can be prescribed Zepbound under the obesity indication, not just Mounjaro under the T2D indication.
- Moderate-to-severe obstructive sleep apnea: In adults with obesity. Zepbound is the first and only FDA-approved prescription medication for this indication, per the Eli Lilly OSA approval press release.
Mounjaro has no approval for either of these uses.
The Molecule: What Tirzepatide Actually Does
Since both brands contain the same active ingredient, understanding what tirzepatide does at the molecular level applies equally to both.
Tirzepatide is the first FDA-approved dual GIP receptor (GIPR) and GLP-1 receptor (GLP-1R) agonist, per the Zepbound prescribing information. Every prior GLP-1 drug on the market — semaglutide, liraglutide, dulaglutide — activates only the GLP-1 receptor. Tirzepatide activates both:
- GLP-1 receptor activation slows gastric emptying, suppresses appetite through hypothalamic signaling, and stimulates glucose-dependent insulin secretion.
- GIP receptor activation enhances insulin secretion in a glucose-dependent manner, suppresses glucagon, and has direct effects on adipose tissue — reducing adipogenesis through fat-tissue GIPR pathways.
The dual mechanism is why tirzepatide produces superior glycemic control compared to prior GLP-1 agonists in T2D (the SURPASS data), and why it produces weight loss that exceeds prior GLP-1 agents by a substantial margin (the SURMOUNT data). There is no need for a head-to-head trial between Zepbound and Mounjaro for weight loss efficacy — they are the same drug.
Dosing: Identical for Both Brands
Both Zepbound and Mounjaro use an identical titration schedule: 2.5 mg subcutaneously once weekly for the first four weeks (a tolerability step only, not an approved maintenance dose), then increasing by 2.5 mg every four or more weeks. The full sequence: 2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg. Maximum dose for both is 15 mg once weekly, per the FDA Zepbound approval press release.
Critical safety rule: Zepbound and Mounjaro must never be used together. They contain the same active ingredient. Using both simultaneously is equivalent to a double dose, the Zepbound prescribing information explicitly states that Zepbound must not be used with other tirzepatide-containing products or with any GLP-1 receptor agonist.
Efficacy: No Head-to-Head Needed
Because Zepbound and Mounjaro contain the same molecule at the same doses, comparing their weight loss efficacy is straightforward: any difference in observed outcomes reflects the different patient populations studied, not the drug itself.
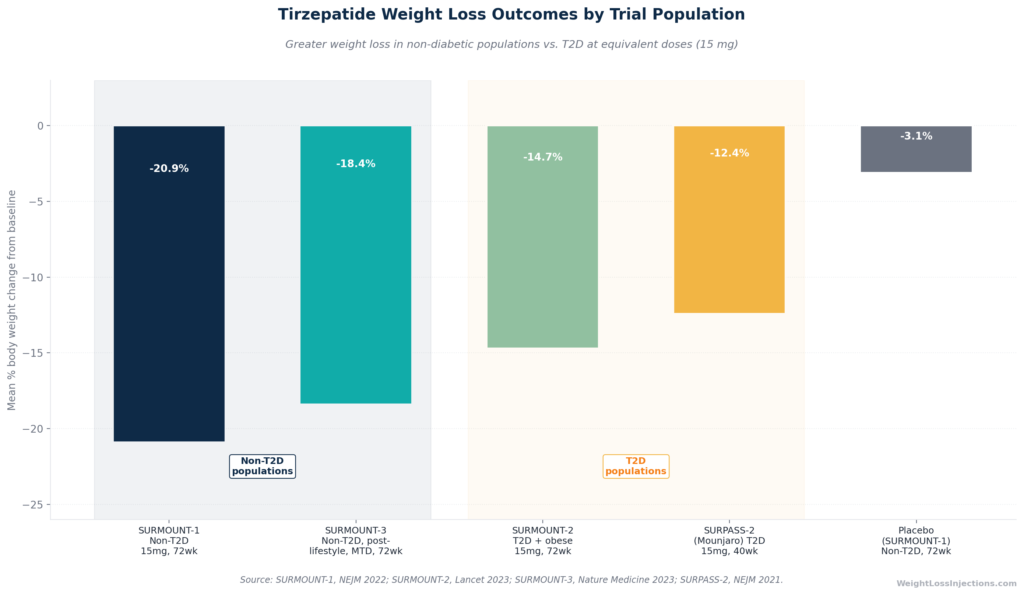
Tirzepatide Weight Loss Outcomes by Trial Population
SURMOUNT Program (Zepbound, Obesity Indication)
The pivotal weight management data comes from the SURMOUNT program, four phase 3 trials in people with obesity or overweight:
- SURMOUNT-1 (72 weeks, non-T2D, 2,539 participants): Tirzepatide 15 mg produced −20.9% mean body weight reduction versus −3.1% on placebo. Fifty-seven percent of patients lost 20% or more of their body weight, per SURMOUNT-1 in the New England Journal of Medicine, 2022.
- SURMOUNT-2 (72 weeks, T2D + obesity, 938 participants): Tirzepatide 15 mg produced −14.7% versus −3.2% placebo — lower than SURMOUNT-1 because T2D patients have greater metabolic resistance to weight loss, per SURMOUNT-2 in The Lancet, 2023.
- SURMOUNT-4 (withdrawal study): Patients who continued tirzepatide lost an additional −5.5% during the maintenance period; those switched to placebo regained +14.0%. Stopping tirzepatide leads to substantial weight regain — obesity is a chronic condition requiring long-term treatment, per SURMOUNT-4 in JAMA, 2023.
SURPASS Program (Mounjaro, T2D Indication)
The SURPASS program enrolled more than 20,000 people with T2D across five global phase 3 registration trials, per the American Diabetes Association SURPASS program summary. Weight loss was not the primary endpoint, glycemic control was, but tirzepatide produced meaningful weight reduction as a secondary outcome:
- SURPASS-2 (40 weeks, T2D): Tirzepatide 15 mg reduced HbA1c by −2.46% versus semaglutide 1 mg. Up to 92% of tirzepatide patients achieved HbA1c <7%. Weight loss was −11.2 kg (−12.4%) at 15 mg versus −4.7 kg with semaglutide 1 mg, per the ADA SURPASS press release.
- SURPASS-4 (52 weeks, T2D with cardiovascular risk): Tirzepatide 15 mg reduced body weight by −13.0% versus +2.2% weight gain with insulin glargine, per the Eli Lilly SURPASS-4 Lancet press release.
The bottom line: when weight loss is your goal, the SURMOUNT data (the Zepbound trials) is the relevant reference. The SURPASS data (the Mounjaro trials) shows what tirzepatide does in a T2D population where glycemic control, not maximum fat loss, was the study objective. Patients with T2D lose less weight on tirzepatide than non-diabetic patients, regardless of which brand label is on the pen.
Insurance Coverage: The Key Practical Difference
This is where the brand distinction stops being a technicality and starts costing real money.
How Insurance Billing Works for Each Brand
When a provider prescribes Mounjaro, the pharmacy claim is billed under type 2 diabetes ICD-10 diagnostic codes (E11.xx). Most commercial health plans that include a diabetes drug benefit will cover Mounjaro for a patient with T2D, subject to standard prior authorization requirements.
When a provider prescribes Zepbound, the claim is billed under obesity ICD-10 diagnostic codes (E66.xx or equivalent). Obesity drug coverage is a separate benefit that many plans offer, but at a meaningfully lower rate than diabetes coverage. Approximately 43–45% of commercial plans cover Zepbound for weight management; roughly 55% of employer-sponsored plans approve it after prior authorization, per Pandameds insurance coverage analysis from March 2026.
This creates a scenario where a patient with both T2D and obesity could, in theory, be covered for Mounjaro under their diabetes benefit but denied for Zepbound under their obesity benefit, even though the drug and dose are identical. This happens because plans administer these as separate benefits with separate formulary decisions.
The OSA Coverage Angle
Zepbound’s December 2024 approval for obstructive sleep apnea introduces a third billing pathway. When prescribed specifically for moderate-to-severe OSA in adults with obesity, the claim may be coded under sleep disorder or respiratory ICD-10 codes, and some plans treat this as a distinct category from both diabetes and obesity, with different formulary placement and often an easier prior authorization pathway. If you have diagnosed OSA with obesity, discussing the OSA indication with your prescriber may open a coverage pathway that the obesity indication alone does not.
Medicare Coverage
Standard Medicare Part D covers neither Zepbound nor Mounjaro for weight loss, Medicare is statutorily prohibited from covering drugs used solely for weight management, per American College of Gastroenterology guidance from April 2025.
Coverage exceptions for Medicare patients:
- Mounjaro for T2D: Medicare Part D plans routinely cover Mounjaro when prescribed for type 2 diabetes. This remains the clearest Medicare coverage pathway for tirzepatide in 2026.
- Zepbound for OSA: Medicare Part D plans may cover Zepbound when prescribed specifically for moderate-to-severe obstructive sleep apnea, subject to individual plan formulary decisions.
- Medicare GLP-1 Bridge (July 1–December 31, 2026): CMS announced a temporary bridge program providing Zepbound at a $50 copayment for eligible Medicare Part D enrollees — BMI ≥35, or BMI ≥27 with clinical criteria. This program operates outside the standard Part D benefit, does not count toward the $2,100 annual out-of-pocket cap, and bridges to the BALANCE Model demonstration beginning in 2027, per KFF analysis from March 2026. Notably, the Medicare GLP-1 Bridge covers Zepbound (obesity indication) — not Mounjaro under this specific program.
Our Top 3 · July 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
2026 Pricing: Where the Two Brands Diverge Most
Both Zepbound and Mounjaro carry a list price (WAC) of approximately $1,086/mo for a 28-day supply at any dose strength, per Eli Lilly’s pricing information. At list price, there is virtually no difference between the two brands. But list price is not what most patients pay, and the self-pay discount structure is dramatically different.

2026 Out-of-Pocket Pricing Comparison: Zepbound vs. Mounjaro
Zepbound Self-Pay via LillyDirect
Eli Lilly built a direct-to-consumer pricing program specifically for Zepbound — it does not have an equivalent for Mounjaro. Via the LillyDirect Self Pay Journey Program, Zepbound is available at substantially below list price for self-pay patients:
- 2.5 mg: $299/mo
- 5 mg: $399/mo
- 7.5 mg, 10 mg, 12.5 mg, or 15 mg: $449/mo (flat, regardless of dose)
These prices apply to single-dose vials and to the KwikPen, a multi-dose device containing four weekly doses per pen that launched February 23, 2026 via LillyDirect, per CNBC reporting on February 23, 2026. Without enrollment in the Self Pay Journey Program, LillyDirect prices are substantially higher (e.g., $599 for 7.5 mg, $699 for 10 mg, $849 for 12.5 mg, $1,049 for 15 mg), per CNBC’s December 1, 2025 report on the LillyDirect price cut.
LillyDirect is also available for retail pickup at Walmart Pharmacy locations nationwide, per Walmart’s October 2025 announcement of the LillyDirect partnership.
Mounjaro and LillyDirect
Mounjaro is not available through the LillyDirect direct-to-consumer self-pay pricing model that Zepbound uses. Mounjaro is dispensed through the traditional pharmacy channel. A self-pay patient filling Mounjaro without insurance coverage would pay approximately the $1,086/mo list price, plus any pharmacy dispensing fees.
Savings Cards: Similar but Not Interchangeable
Both brands offer manufacturer savings cards for commercially insured patients, and both can bring the monthly cost down to as low as $25/mo with a covered commercial insurance benefit:
- Zepbound savings card (covered benefit): As low as $25/mo for up to 13 fills in 2026, with a maximum annual benefit of approximately $1,300. Available to U.S. and Puerto Rico residents with commercial drug insurance. Government beneficiaries (Medicare, Medicaid, VA, TRICARE) are excluded, per 2026 savings card terms tracking on community sources.
- Zepbound savings card (non-covered benefit): As low as $499/mo for patients with commercial insurance but no obesity drug coverage benefit, up to 7 fills per year, per PrescriberPoint savings program details.
- Mounjaro savings card: Available for commercially insured patients with T2D coverage. Brings cost to approximately $25/mo with covered benefit. Not usable for off-label weight management use, and government beneficiaries are excluded.
The savings cards are not interchangeable. You cannot use a Zepbound savings card on a Mounjaro prescription, or vice versa. Each card is tied to the brand and the indication.
What This Means for Self-Pay Patients
If you are a self-pay patient without insurance coverage and your goal is weight loss, not T2D management, the financial calculation is unambiguous: Zepbound via LillyDirect is the only branded tirzepatide option with below-list self-pay pricing. A self-pay patient prescribed Mounjaro for off-label weight loss would pay roughly $1,086/mo at the pharmacy counter. The same patient prescribed Zepbound and using LillyDirect pays $299–$449/mo for the identical drug at the identical dose.
Can You Switch From Mounjaro to Zepbound?
Yes, and it is clinically straightforward. But it requires a new prescription, and there are insurance implications to understand before you make the switch.
Clinical Considerations
Because both brands contain the same tirzepatide at the same dose, switching is a dose-equivalent transition in most cases. A patient on Mounjaro 10 mg/wk switching to Zepbound for weight management would typically continue at the same dose under clinical guidance, rather than restarting the titration from 2.5 mg. Clinical judgment applies, some prescribers prefer a brief step-down and re-titration to confirm tolerability is maintained, especially if the patient had GI side effects at the current dose. Discuss timing with your prescriber.
There is no washout period required for a same-molecule switch between Mounjaro and Zepbound. The drugs are identical; you do not need to wait weeks between the last Mounjaro dose and the first Zepbound dose the way you would if switching between mechanistically different agents.
What the Pharmacy Requires
Despite containing the same drug, Mounjaro and Zepbound cannot be substituted at the pharmacy. They are different NDAs, different brand names, and require different prescriptions. Your pharmacist cannot legally fill a Zepbound prescription with Mounjaro, or vice versa, even though the active ingredient is identical. You need a new Zepbound prescription written by your provider.
Insurance Re-Authorization
Switching brands almost always triggers a new prior authorization process. A prior authorization issued for Mounjaro under your T2D benefit does not transfer to Zepbound under your obesity benefit, those are different benefits administered under different formulary rules. Before switching, confirm with your insurer:
- Does your plan cover Zepbound for weight management or OSA?
- What are the prior authorization criteria (BMI threshold, required comorbidities, documentation of prior lifestyle intervention)?
- How long does the prior authorization review typically take?
Starting the insurance process before the prescription is written, not after, avoids a coverage gap.
Why Someone Prescribed Mounjaro Off-Label for Weight Loss Should Switch to Zepbound
If your provider has been prescribing Mounjaro off-label for weight loss because you do not have T2D, switching to Zepbound puts your prescription on-label and positions you correctly for:
- Insurance coverage under your obesity benefit (if your plan covers it)
- Access to the Zepbound savings card
- Access to LillyDirect self-pay pricing ($299–$449/mo)
- Eligibility for the Medicare GLP-1 Bridge program if you have Medicare (Zepbound only, July–December 2026)
The drug does not change. Your access to financial assistance and coverage does.
Device Formats: One More Difference
The physical delivery devices differ between the two brands in one meaningful way for self-pay patients.
Zepbound is available in three formats as of April 2026:
- Single-dose auto-injector pen — prefilled, color-coded by dose strength, one pen equals one weekly dose; available in all six strengths through retail pharmacies and LillyDirect.
- Single-dose vial — requires a separate syringe and needle; available in all six strengths through LillyDirect; lower self-pay pricing applies.
- Multi-dose KwikPen — contains four weekly doses per pen (one month of treatment); launched February 23, 2026; available only through LillyDirect for self-pay patients, per CNBC Feb 23, 2026. Not yet available through traditional pharmacies as of April 2026.
Mounjaro is available in two formats:
- Single-dose auto-injector pen — available through traditional pharmacies in all six strengths.
- KwikPen — the multi-dose pen format; available through pharmacy distribution for Mounjaro. Note: the Mounjaro KwikPen is dispensed through the standard pharmacy channel at list price, not through a LillyDirect self-pay program.
For patients who prefer an auto-injector pen over a vial-and-syringe approach but want LillyDirect pricing, the Zepbound KwikPen launched in February 2026 provides that combination — a convenience unavailable with Mounjaro’s self-pay economics.
Who Should Ask for Which Brand?
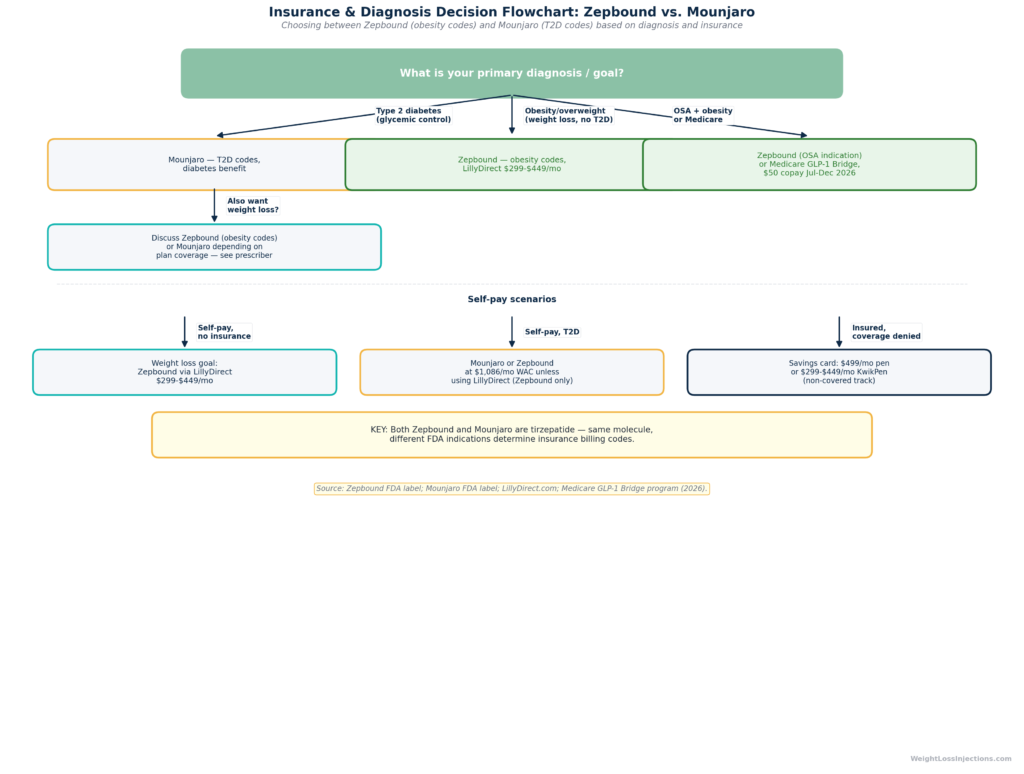
Insurance and Diagnosis Decision Flowchart for Zepbound vs. Mounjaro
Ask for Mounjaro If:
- Your primary diagnosis is T2D and glycemic control is the primary therapeutic goal. Mounjaro’s SURPASS data specifically establishes tirzepatide’s efficacy in reducing HbA1c for T2D patients. Your insurer covers it under the diabetes benefit. This is Mounjaro’s clinical home.
- Your insurer covers Mounjaro under a diabetes benefit but does not cover Zepbound under an obesity benefit. This is a real scenario. If your plan covers Mounjaro with a $25 copay via savings card but does not cover Zepbound at all, Mounjaro may be the financially rational choice — even if weight loss is also a goal — while you work on a Zepbound prior authorization appeal.
- You are a Medicare beneficiary with T2D only (no obesity comorbidities meeting GLP-1 Bridge criteria) and your plan covers Mounjaro for T2D under Part D.
Ask for Zepbound If:
- Your primary goal is weight loss, with or without T2D. Zepbound is the FDA-approved on-label option. Even if you have T2D, T2D is a qualifying comorbidity for the Zepbound weight management indication, you do not have to forgo Zepbound just because you also have diabetes.
- You have moderate-to-severe OSA with obesity. Zepbound is the only FDA-approved medication for this indication. In SURMOUNT-OSA, 42% of tirzepatide patients with no PAP therapy baseline no longer had moderate-to-severe OSA at 52 weeks, versus 16% on placebo, per the Eli Lilly OSA approval press release. The OSA indication may also open a separate insurance coverage pathway with fewer prior authorization hurdles than the obesity indication.
- You are self-pay. LillyDirect self-pay pricing ($299–$449/mo) is only available for Zepbound. There is no equivalent program for Mounjaro.
- You are a Medicare beneficiary eligible for the GLP-1 Bridge (BMI ≥35 or ≥27 with clinical criteria) during the July–December 2026 program period. The Bridge covers Zepbound, per KFF analysis from March 2026.
- You want to get your prescription on-label. If a prior provider was prescribing Mounjaro off-label for your weight without T2D, switching to Zepbound puts you on the correct regulatory footing for coverage access and financial assistance programs.
A Note on International Availability
Outside the United States, the brand-name differentiation may not apply in the same way. In some markets, tirzepatide is approved under a single brand for multiple indications, or the approval timeline for weight management has lagged behind the T2D approval. Patients traveling or obtaining prescriptions internationally should confirm which brand and indication are locally approved. This article covers U.S. FDA indications and U.S. pricing only.
A Note on Compounded Tirzepatide
Patients researching this topic may encounter references to “compounded tirzepatide”, a lower-cost alternative marketed by telehealth companies during the period when tirzepatide was on the FDA drug shortage list. The shortage window that permitted this compounding is closed. The 503A pharmacy window closed February 18, 2025; the 503B outsourcing facility window closed March 19, 2025, per FDA clarification on compounding policies. As of April 2026, any entity mass-marketing compounded tirzepatide is operating outside these closed windows and may be subject to federal enforcement action, per Pharmacy Times reporting from February 2026. The only legitimate tirzepatide products available in the United States are Zepbound (NDA 217806) and Mounjaro (NDA 215866).
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: The question of “Zepbound vs. Mounjaro” is really a question about your diagnosis, your insurance, and your goals, not about the drug itself. At the molecular level, there is nothing to debate: these products are the same tirzepatide manufactured by the same company to the same standards. The difference is entirely in the FDA label, and that difference cascades into meaningful financial and access consequences.
For patients without T2D who want weight loss: ask for Zepbound. There is no clinical reason to be prescribed Mounjaro off-label when Zepbound is the on-label option with better insurance and self-pay access. Mounjaro off-label for weight loss in a non-diabetic patient is the worst of both worlds, no LillyDirect pricing, no applicable savings card, no insurance coverage pathway.
For patients with T2D who also want meaningful weight loss: the conversation is more nuanced. Mounjaro is the on-label T2D option and may be covered under your diabetes benefit. But Zepbound is also available, T2D qualifies as a comorbidity for the Zepbound obesity indication, and your provider should evaluate both coverage pathways. In many cases, a plan will cover Mounjaro under T2D and Zepbound under obesity as separate benefits, so you may have more options than you realize.
For Medicare patients: Mounjaro remains the clearest standard coverage path if you have T2D. But the GLP-1 Bridge (July–December 2026) is a time-limited opportunity to access Zepbound at $50/mo, worth discussing with your prescriber before the program closes.
One thing is not up for debate: the two brands cannot be used at the same time. If you are on one, do not take the other. The prescribing information could not be clearer on this point.
If you want to understand which option fits your specific situation, [service detail] at WeightLossInjections.com connects you with a licensed clinician for [$X/month] to evaluate your diagnosis, insurance plan, and pricing options.
Frequently Asked Questions
At the molecular level, yes. Both Zepbound and Mounjaro contain tirzepatide, the same active ingredient, the same 39-amino acid peptide, the same dose strengths (2.5 mg through 15 mg), and the same once-weekly subcutaneous injection schedule. They are manufactured by Eli Lilly to identical specifications, per the Zepbound prescribing information. The difference is regulatory: Zepbound is approved under NDA 217806 for chronic weight management and obstructive sleep apnea; Mounjaro is approved under NDA 215866 for type 2 diabetes only.
No. This is explicitly contraindicated. Both products contain tirzepatide, taking them simultaneously is a double dose of the same active ingredient. The Zepbound prescribing information states clearly that Zepbound must not be used with other tirzepatide-containing products. Combining them increases the risk of severe adverse effects including pancreatitis, acute kidney injury from dehydration, and severe hypoglycemia if you are also using insulin or sulfonylureas. If you are on one, you should not be on the other, and transitioning between them does not require a washout period, just a single prescription change.
Several reasons. If you have T2D, your insurer may cover Mounjaro under the diabetes benefit but not Zepbound under the obesity benefit, Mounjaro may simply be the covered option. Some providers default to Mounjaro from prior prescribing habits established before Zepbound launched in late 2023. In other cases, a patient may have failed to meet the BMI or comorbidity criteria documented for a Zepbound prior authorization. If your primary goal is weight loss and you do not have T2D, it is worth asking your provider whether a Zepbound prescription makes more sense, Zepbound is the on-label option for weight management, carries better self-pay pricing, and opens access to the Zepbound savings card and LillyDirect, per the FDA Zepbound approval press release.
Approximately 43–45% of commercial plans cover Zepbound for the weight management indication (BMI ≥30 or ≥27 with a qualifying comorbidity), rising to roughly 55% at employer-sponsored plans after prior authorization, per Pandameds insurance analysis from March 2026. Coverage typically requires documented BMI, a record of prior lifestyle intervention, and prior authorization. If your plan denies coverage, the non-covered savings card brings cost to as low as $499/mo, and LillyDirect self-pay starts at $299/mo, substantially below the $1,086/mo list price. Medicare Part D does not cover Zepbound for weight management under standard benefits, per American College of Gastroenterology guidance from April 2025, though the temporary GLP-1 Bridge (July–December 2026) provides $50 copay access for eligible enrollees, per KFF March 2026.
No. LillyDirect requires a valid prescription for Zepbound. You must have a provider evaluation and a prescription before LillyDirect can dispense the medication. LillyDirect partners with healthcare providers and telehealth services, but it does not prescribe, it dispenses. If you do not have a prescribing provider, a licensed telehealth service can evaluate your eligibility and write a Zepbound prescription that routes to LillyDirect for fulfillment. WeightLossInjections.com offers [service detail] for exactly this purpose.
The SURMOUNT-4 withdrawal study showed that stopping tirzepatide leads to substantial weight regain. Patients switched from tirzepatide to placebo after a 36-week open-label period regained +14.0% of their body weight over the following 52 weeks, while patients who continued tirzepatide lost an additional −5.5%, per SURMOUNT-4 in JAMA, 2023. Overall at week 88, the continued-tirzepatide group maintained −25.3% total weight change versus −9.9% in the group who stopped. This is not a flaw in the medication, it reflects that obesity is a chronic condition driven by persistent physiological mechanisms, and long-term treatment is required to maintain the benefit. The same principle applies equally to Zepbound and Mounjaro since the drug is the same.
