![Unbranded [pillar-drug-class] injection pen on a neutral background — WeightLossInjections.com editorial hero](https://weightlossinjections.com/wp-content/uploads/2026/05/hero_zepbound_c4_compare-1200x675.png)
Zepbound vs. Ozempic Head-to-Head Overview
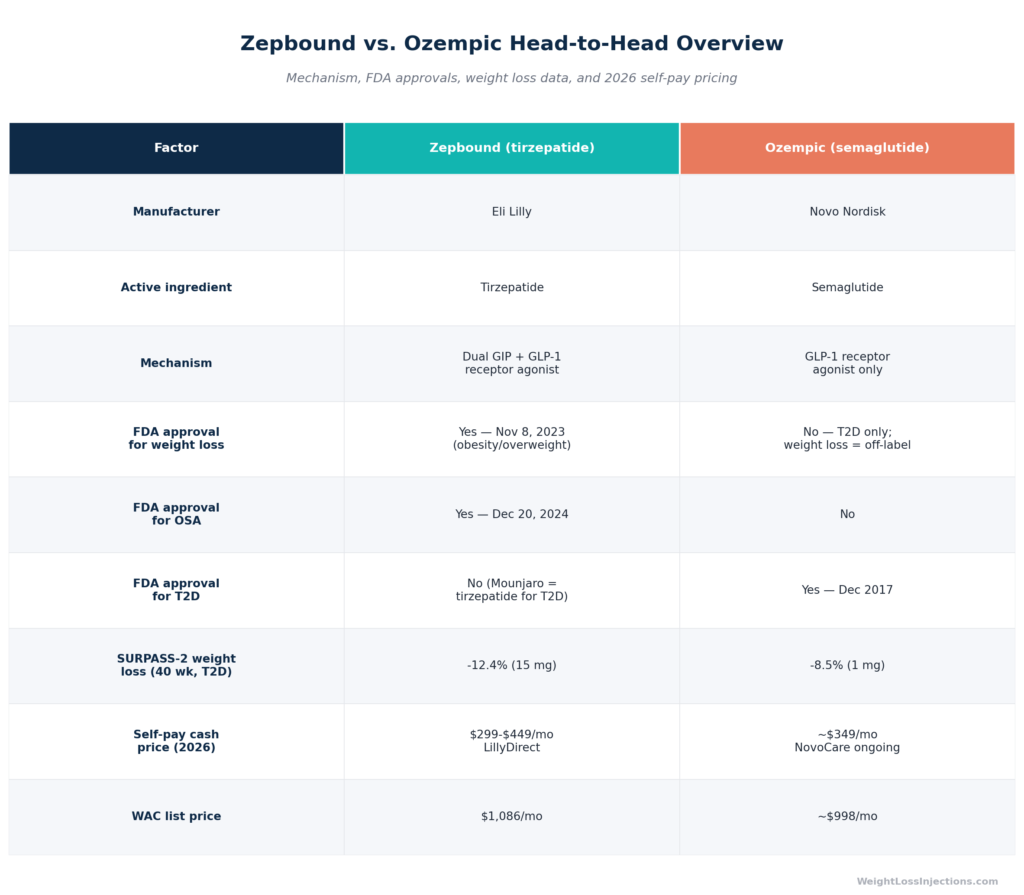
Zepbound (tirzepatide, Eli Lilly) is FDA-approved for chronic weight management and obstructive sleep apnea. Ozempic (semaglutide, Novo Nordisk) is FDA-approved for type 2 diabetes only, using it for weight loss is off-label. In the only direct head-to-head trial in a T2D population (SURPASS-2), tirzepatide 15 mg produced 12.4% weight loss versus 8.5% for semaglutide 1 mg at 40 weeks.
For weight loss specifically, the FDA-approved semaglutide option is Wegovy (2.4 mg), not Ozempic. Self-pay pricing in 2026 runs $299–$449/mo for Zepbound via LillyDirect versus $349/mo ongoing for Ozempic via NovoCare.
What Is Zepbound (Tirzepatide)?
Mechanism: Dual GIP + GLP-1 Receptor Agonism
Tirzepatide, the active ingredient in Zepbound, is the first FDA-approved drug to simultaneously activate two incretin hormone receptors: the glucose-dependent insulinotropic polypeptide receptor (GIPR) and the glucagon-like peptide-1 receptor (GLP-1R), per the Zepbound prescribing information. That dual mechanism is the defining molecular difference between Zepbound and Ozempic.
Here is what each receptor pathway contributes:
- GLP-1R activation slows gastric emptying, reduces appetite through central hypothalamic signaling, and stimulates glucose-dependent insulin secretion. This is the pathway Zepbound and Ozempic share.
- GIPR activation enhances insulin secretion in a glucose-dependent manner, suppresses glucagon, and acts directly on adipose tissue to reduce adipogenesis — metabolic effects that semaglutide’s single-receptor approach cannot replicate, per the Zepbound prescribing information.
The proposed explanation for tirzepatide’s greater weight-loss results is not simply “more GLP-1 signal” but a qualitatively different, broader hormonal response that activates downstream metabolic pathways semaglutide does not reach. Tirzepatide is a 39-amino-acid synthetic peptide with a C20 fatty diacid moiety that enables once-weekly dosing via albumin binding and a half-life of approximately 5–6 days, per the FDA pharmacology review NDA 217806.
FDA Approvals for Zepbound
Zepbound holds two distinct FDA approvals — a combination no other weight-loss medication can claim:
- Chronic weight management (November 8, 2023): Approved as an adjunct to a reduced-calorie diet and increased physical activity for adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbid condition, per the FDA Zepbound approval press release.
- Moderate-to-severe obstructive sleep apnea (December 20, 2024): Zepbound is the first and only prescription medication approved for this indication in adults with obesity, per the Eli Lilly OSA approval press release. Ozempic holds neither of these approvals.
Dosing
Zepbound starts at 2.5 mg subcutaneously once weekly (a tolerability step, not a therapeutic dose) and titrates in 2.5 mg increments every four weeks: 2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg. Maximum dose is 15 mg once weekly. Maintenance doses for weight management are 5, 10, or 15 mg; the OSA indication uses 10 or 15 mg, per the Zepbound prescribing information. Three device formats exist as of April 2026: single-dose auto-injector pen, single-dose vial, and the multi-dose KwikPen (launched February 23, 2026), per CNBC Feb 23, 2026.
What Is Ozempic (Semaglutide)?
Mechanism: GLP-1 Receptor Agonism Only
Semaglutide, the active ingredient in Ozempic, is a mono GLP-1 receptor agonist. It mimics the incretin hormone GLP-1, slowing gastric emptying, suppressing appetite, and stimulating glucose-dependent insulin release. It does not activate the GIP receptor. This single-receptor design produces meaningful but categorically lower weight-loss outcomes compared to tirzepatide in head-to-head data, as detailed below.
Ozempic was first approved by the FDA for type 2 diabetes in December 2017 (NDA 209637). A cardiovascular risk reduction indication was subsequently added for adults with T2D and established cardiovascular disease, based on the SUSTAIN-6 trial outcomes. As of April 2026, Ozempic is approved at doses up to 2 mg for T2D adults.
Ozempic Is NOT Approved for Weight Loss
This is the most important regulatory distinction in this comparison: Ozempic is not FDA-approved for weight loss or obesity management. Its label covers type 2 diabetes and cardiovascular risk reduction only.
The FDA-approved semaglutide formulation for weight management is Wegovy, which delivers 2.4 mg semaglutide weekly — a higher dose than Ozempic’s maximum 2 mg label. Wegovy was approved for obesity on June 4, 2021. Patients and providers who use Ozempic for weight loss are using it off-label, which is legally permissible but means the indication is not supported by the FDA’s formal risk-benefit review for that use case.
The off-label status carries practical consequences: commercial insurers who cover weight-loss medications do so for on-label drugs like Zepbound and Wegovy, not for Ozempic prescribed off-label for obesity. This is not a minor technical distinction — it is a primary driver of real-world coverage denials.
Ozempic Dosing
Ozempic starts at 0.25 mg once weekly (initiation dose), escalates to 0.5 mg, then 1 mg, and (for T2D patients requiring additional glycemic control) 2 mg. The escalation schedule uses 4-week minimum intervals between dose increases, per the Ozempic FDA prescribing information NDA 209637. By comparison, Wegovy escalates to a 2.4 mg maximum, a dose not available with Ozempic’s labeled use.
FDA Indications Compared: Why Approval Status Matters
FDA Indication Comparison Table
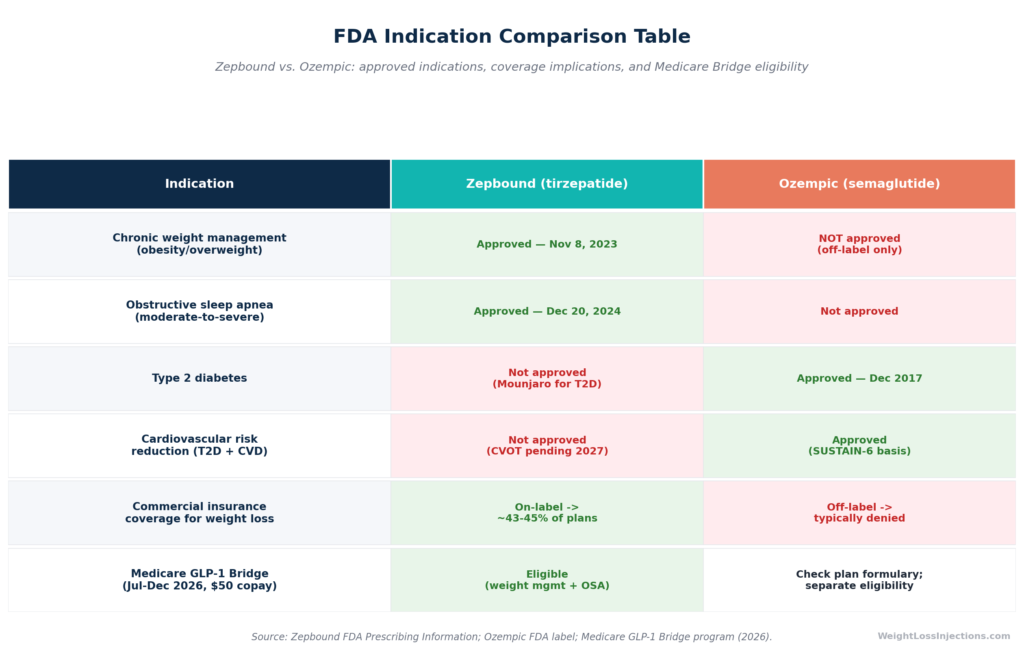
The table below shows how the approval landscape translates into real-world coverage access:
| Indication | Zepbound | Ozempic |
|---|---|---|
| Chronic weight management | Approved — Nov 8, 2023 | NOT approved (off-label) |
| Obstructive sleep apnea | Approved — Dec 20, 2024 | Not approved |
| Type 2 diabetes | Not approved (→ Mounjaro) | Approved — Dec 2017 |
| CV risk reduction (T2D + CVD) | Not approved (CVOT ongoing) | Approved |
| Commercial insurance (weight loss) | On-label → ~43–45% coverage | Off-label → typically denied |
| Medicare GLP-1 Bridge (Jul–Dec 2026) | Eligible at $50 copay | Check individual plan |
Sources: FDA Zepbound approval press release; Eli Lilly OSA approval press release; Pandameds insurance coverage analysis, March 2026.
Why On-Label Approval Changes the Insurance Equation
Zepbound’s on-label weight management approval means that commercial insurers considering an anti-obesity medication (AOM) benefit can add Zepbound to their formulary as a covered drug with a prior-authorization pathway. Approximately 43–45% of commercial plans currently cover Zepbound for weight management, with employer-sponsored plans showing approximately 55% approval after prior authorization, per Pandameds insurance coverage analysis.
Ozempic used off-label for weight loss lacks this pathway entirely. An insurer has no regulatory scaffold to justify covering an off-label indication, and standard coverage policy language directs weight-loss-seeking patients to FDA-approved alternatives. In practice, attempting to get a commercial plan to cover Ozempic off-label for obesity, rather than Zepbound or Wegovy on-label, is almost always a coverage denial.
The OSA Approval: A Unique Clinical and Coverage Pathway
Zepbound’s December 2024 OSA approval creates a coverage route that Ozempic cannot access. Medicare Part D plans may cover Zepbound when it is prescribed specifically for moderate-to-severe obstructive sleep apnea in adults with obesity, an indication entirely absent from Ozempic’s label. For patients with comorbid obesity and OSA, this is clinically and financially meaningful.
The SURMOUNT-OSA trial data underpinning this approval showed a reduction in apnea-hypopnea index (AHI) of −25.3 events per hour with tirzepatide versus −5.3 with placebo (no-PAP therapy arm), and 42% of tirzepatide patients no longer had moderate-to-severe OSA at 52 weeks versus 16% on placebo, per the Eli Lilly OSA press release.
Ozempic’s Cardiovascular Advantage
Ozempic holds FDA approval for cardiovascular risk reduction in adults with type 2 diabetes and established cardiovascular disease, an indication Zepbound does not yet have. The SUSTAIN-6 trial demonstrated a statistically significant reduction in major adverse cardiovascular events (MACE) for patients on semaglutide, per the Ozempic prescribing information. Zepbound’s CVOT (cardiovascular outcomes trial) is ongoing with results expected approximately 2027; it is not yet eligible to claim a formal CV indication.
This means that for patients with established cardiovascular disease who also have type 2 diabetes, Ozempic’s on-label cardiovascular protection is a clinically documented benefit that Zepbound cannot yet match.
Head-to-Head Weight Loss Efficacy: SURPASS-2
The most scientifically valid comparison of tirzepatide and semaglutide for weight loss comes from the SURPASS-2 trial, the only study to directly randomize patients to both drugs. Understanding what this trial does and does not show is essential for interpreting efficacy claims about either medication.
SURPASS-2 Trial Design and Limitations
SURPASS-2 was a phase 3, open-label, active-controlled trial that randomized 1,879 adults with type 2 diabetes and inadequate glycemic control on metformin to tirzepatide 5 mg, 10 mg, or 15 mg, or semaglutide 1 mg, once weekly for 40 weeks. The comparator was semaglutide 1 mg, not semaglutide’s maximum T2D dose of 2 mg, and not Wegovy’s weight-management dose of 2.4 mg. This is a critical limitation: the trial was designed to compare glycemic agents in T2D, not to test weight-loss maximum doses. The results favor tirzepatide, but semaglutide’s actual weight-loss ceiling (at 2.4 mg) was not tested in this head-to-head design, per the ADA SURPASS program summary.
Weight Loss Results From SURPASS-2
Despite the dose caveat, the SURPASS-2 weight-loss data is the best available head-to-head evidence:
| Treatment | Mean % Body Weight Change (40 wks) | Mean kg Change |
|---|---|---|
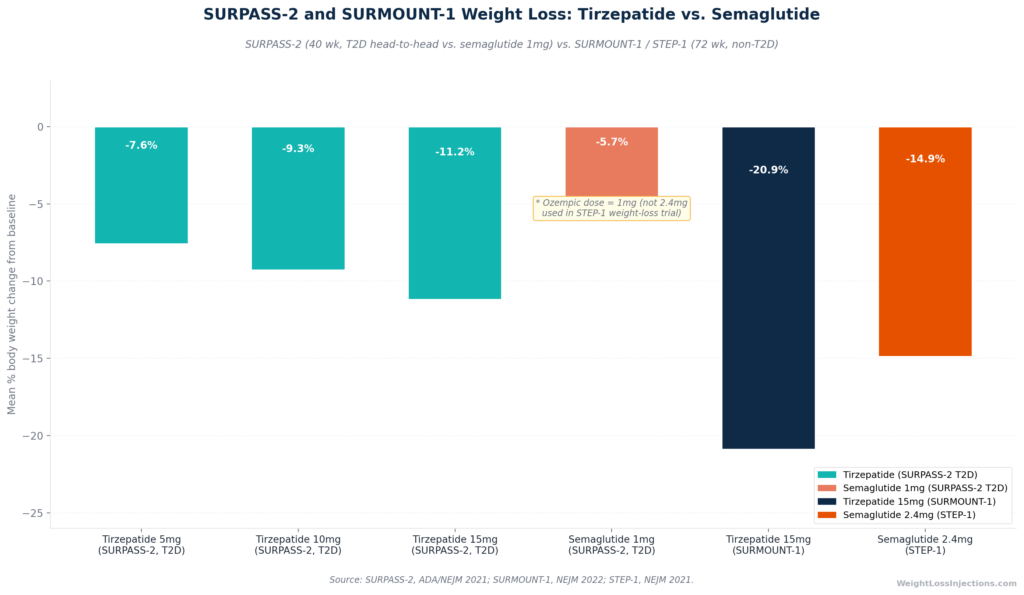
| Tirzepatide 5 mg | −7.6% | ~−6.2 kg |
| Tirzepatide 10 mg | −9.3% | ~−7.6 kg |
| Tirzepatide 15 mg | −11.2% | ~−9.2 kg |
| Semaglutide 1 mg | −5.7% | ~−4.7 kg |
Source: ADA SURPASS program summary. All three tirzepatide doses delivered statistically superior weight loss versus semaglutide 1 mg (p<0.001 for each comparison). The maximum tirzepatide dose (15 mg) produced approximately double the weight loss of the semaglutide 1 mg comparator.
Separately, the SURPASS-2 glycemic data showed that up to 92% of tirzepatide patients achieved HbA1c below 7%, versus a lower proportion on semaglutide, per ADA SURPASS program summary. For patients managing both T2D and obesity, tirzepatide’s dual glycemic and weight benefit in the T2D population is the strongest evidence base for the choice.
Putting SURPASS-2 in Context: SURMOUNT-1 and STEP-1
For non-diabetic patients, the relevant pivotal trials are SURMOUNT-1 (tirzepatide) and STEP-1 (semaglutide 2.4 mg, the Wegovy dose). These were run in different populations and different years — they are not interchangeable comparisons — but they provide useful context for upper-bound efficacy:
- SURMOUNT-1 (tirzepatide 15 mg, 72 weeks, no T2D): −20.9% average weight loss, with 57% of patients losing ≥20% of body weight, per NEJM 2022, Jastreboff et al.
- STEP-1 (semaglutide 2.4 mg / Wegovy, 68 weeks, no T2D): −14.9% average weight loss, per the STEP program. This is the Wegovy dose — not the Ozempic dose.
The meaningful takeaway: Ozempic at its labeled maximum of 2 mg in T2D patients produced 5.7% weight loss in SURPASS-2. Tirzepatide at 15 mg produced 20.9% in a non-T2D population (SURMOUNT-1). These are different populations at different doses, but the direction of effect is consistent across every available data point.
SURPASS-2 and SURMOUNT-1 Weight Loss Bar Chart
SURMOUNT-2: Tirzepatide in T2D for Weight Loss
For patients with type 2 diabetes seeking weight management specifically, SURMOUNT-2 provides direct data on tirzepatide’s weight-loss efficacy in that population. The phase 3 trial enrolled 938 adults with BMI ≥27 and T2D; at 72 weeks, tirzepatide 15 mg produced −14.7% average weight loss versus −3.2% placebo, per Lancet 2023. In the same trial, 83% of patients on 15 mg lost ≥5% of body weight, and 49% of patients on tirzepatide achieved normoglycemic HbA1c below 5.7%, per the ACC SURMOUNT-2 summary. No comparable weight-loss-powered trial of Ozempic in T2D patients produces numbers in this range at Ozempic’s licensed doses.
Cost and Access in 2026
List Prices (WAC)
At wholesale acquisition cost, both drugs carry substantial sticker prices that reflect the rebate infrastructure of U.S. drug pricing rather than what most patients actually pay:
- Zepbound: $1,086/mo for a 28-day supply (all strengths, 2.5–15 mg), per Eli Lilly pricing information, verified April 2026
- Ozempic: approximately $998/mo WAC as of April 2026 (all doses). Novo Nordisk announced a list-price reset to $675/mo for all semaglutide forms — including Ozempic — effective January 1, 2027, per U.S. News & World Report, February 2026
Neither list price is what self-pay patients pay in practice.
Self-Pay Programs: LillyDirect vs. NovoCare
This is where the real-world cost comparison lives for patients without insurance coverage.
Zepbound via LillyDirect (Self Pay Journey Program, effective December 1, 2025):
- 2.5 mg: $299/mo
- 5 mg: $399/mo
- 7.5 mg, 10 mg, 12.5 mg, and 15 mg: $449/mo each
Enrollment in the Self Pay Journey Program is required for these prices. Without enrollment, LillyDirect prices are substantially higher (e.g., $1,049/mo for 15 mg outside the program). Prices apply to single-dose vials and the new KwikPen, per CNBC Dec 1, 2025 and CNBC Feb 23, 2026.
Ozempic via NovoCare Pharmacy (self-pay, April 2026):
| Dose | Monthly Cost |
|---|---|
| 0.25 mg or 0.5 mg (introductory, new patients, through June 30, 2026) | $199/mo for first 2 fills |
| 0.25 mg, 0.5 mg, or 1 mg (ongoing self-pay) | $349/mo |
| 2 mg | $499/mo |
Source: NovoCare Pharmacy savings page; Novo Nordisk November 2025 introductory offer press release. Government beneficiaries (Medicare, Medicaid, VA, TRICARE) are excluded from NovoCare self-pay pricing.
For weight loss patients comparing the two side-by-side: At maintenance doses, Zepbound’s $449/mo (LillyDirect, 7.5–15 mg) exceeds Ozempic’s NovoCare $349/mo for lower doses — but Zepbound delivers consistently greater weight loss in available data. On a cost-per-pound-lost basis over a 12-month course, tirzepatide’s superior efficacy can offset its higher monthly cost for many patients.
With Commercial Insurance and Savings Cards
Commercially insured patients with formulary coverage can access significant savings through manufacturer programs:
- Zepbound: As low as $25/mo with commercial insurance coverage and the Lilly savings card (2026 terms: maximum savings ~$1,300 annually, up to 13 fills per calendar year, U.S. and Puerto Rico residents), per Zepbound savings program details, verified April 2026
- Ozempic: As low as $25/mo with commercial insurance coverage of the diabetes indication and the Novo Nordisk savings card (maximum $100/mo savings, valid up to 48 months), per the Ozempic savings page. The $25 copay path for Ozempic requires a T2D diagnosis on the plan — off-label weight-loss use does not qualify.
- For commercially insured patients without formulary coverage: Zepbound’s non-covered savings card runs ~$499/mo (annual maximum benefit ~$3,283, up to 7 fills per year), per PrescriberPoint Zepbound savings data
Medicare Coverage
Standard Medicare Part D does not cover either drug for weight management — Medicare is statutorily prohibited from covering drugs used solely for weight loss, per American College of Gastroenterology guidance, April 2025.
Important 2026 Medicare coverage pathways:
- Zepbound for OSA: Medicare Part D plans may cover Zepbound when prescribed for moderate-to-severe obstructive sleep apnea with obesity, subject to individual plan formulary — a coverage route with no Ozempic equivalent.
- Ozempic for T2D and cardiovascular risk: Medicare Part D covers Ozempic for its diabetes and cardiovascular indications under normal benefit rules, subject to the $2,100 annual out-of-pocket cap effective 2026 under the Inflation Reduction Act.
- Medicare GLP-1 Bridge (July 1–December 31, 2026): CMS announced a temporary program covering Zepbound and Wegovy at a $50 copayment for eligible Part D enrollees (BMI ≥35, or ≥27 with clinical criteria). Ozempic is a T2D drug, not an obesity drug under Medicare’s classification — patients seeking GLP-1 coverage for weight loss under the Bridge program will be directed to Zepbound or Wegovy, not Ozempic. The Bridge program bridges to the BALANCE Model demonstration beginning 2027, per KFF analysis, March 2026.
| Access Scenario | Zepbound | Ozempic |
|---|---|---|
| WAC list price | $1,086/mo | ~$998/mo |
| Self-pay program (starter dose) | $299/mo (2.5 mg, LillyDirect) | $199/mo intro / $349 ongoing (NovoCare) |
| Self-pay program (maintenance) | $449/mo (7.5–15 mg, LillyDirect) | $349/mo (0.5–1 mg) / $499/mo (2 mg, NovoCare) |
| Commercial insurance + savings card | As low as $25/mo (covered) | As low as $25/mo (T2D coverage only) |
| Medicare weight-loss Bridge (Jul–Dec 2026) | $50 copay (eligible) | Not eligible for weight-loss Bridge |
| Medicare OSA coverage | Eligible (Dec 2024 indication) | Not eligible |
Sources: CNBC Dec 1, 2025; NovoCare Pharmacy; KFF Medicare GLP-1 Bridge analysis.
Our Top 3 · July 2026
The best GLP-1 providers right now
Independently reviewed. Ranked by price, medication access, provider quality, and patient outcomes.
Renew GLP
Personalized GLP-1, GIP plans: Semaglutide & Tirzepatide.
Medvi
No membership or hidden fees. Everything you need is included.
Trimi
US-licensed clinicians and shipped to your door, from $99/mo.
Side-Effect Profile: How They Compare
Both drugs produce side effects typical of the GLP-1 incretin class — predominantly gastrointestinal reactions that are most prominent during dose escalation and usually diminish once a stable maintenance dose is reached.
GI Adverse Events (From FDA Labels)
| Adverse Reaction | Zepbound 15 mg | Ozempic 2 mg (T2D) |
|---|---|---|
| Nausea | 28% | ~15–20% |
| Diarrhea | 23% | ~8–9% |
| Vomiting | 13% | Reported; lower than Zepbound |
| Constipation | 11% | Reported; lower than Zepbound |
Source: Zepbound prescribing information, Table 1; Ozempic prescribing information NDA 209637. Overall GI adverse events occurred in 56% of pooled Zepbound patients versus 30% placebo in the SURMOUNT registration studies, per Zepbound prescribing information. Zepbound’s higher GI event rates at maximum dose partially reflect its greater pharmacological activity, more receptor engagement drives both more weight loss and more nausea.
In SURPASS-2, tirzepatide’s GI profile at maintenance doses was consistent with SURMOUNT trial data. The head-to-head discontinuation rates were not the primary endpoint of SURPASS-2, but the trial did not signal a meaningful tolerability disadvantage for tirzepatide versus semaglutide 1 mg, per ADA SURPASS program summary.
Shared Serious Risks
Both Zepbound and Ozempic carry a black box warning for thyroid C-cell tumors based on rodent data. The human relevance is unknown, but both drugs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2), per the Zepbound prescribing information and Ozempic prescribing information. This parallel warning applies to both drugs and to the entire GLP-1 receptor agonist class.
Additional serious risks shared by both agents:
- Pancreatitis — discontinue if suspected; neither drug has been studied in patients with prior pancreatitis history
- Gallbladder disease — cholelithiasis and cholecystitis reported with GLP-1 class agents
- Acute kidney injury (AKI) — dehydration from nausea, vomiting, and diarrhea can precipitate AKI; maintain adequate hydration
- Hypoglycemia — substantially elevated risk when combined with insulin or sulfonylureas; monitor blood glucose and consider dose reduction of concomitant agents
- Diabetic retinopathy worsening — observed in T2D patients on semaglutide (Ozempic); monitor
- Suicidal behavior/ideation — class-level monitoring requirement; causal relationship not established
Per the FDA Zepbound approval press release, neither drug should be combined with the other or with any other GLP-1 receptor agonist (liraglutide, dulaglutide, exenatide) — tirzepatide activates the same GLP-1R that semaglutide targets, making combination use a pharmacological and safety concern.
Zepbound-Specific Safety Considerations
The Zepbound label carries specific guidance for patients on oral contraceptives: use backup or alternative contraception for four weeks after initiation and four weeks after each dose escalation, because delayed gastric emptying may reduce oral drug absorption, per the Zepbound prescribing information. This applies to any oral medication with gastric-emptying-sensitive absorption. Patients undergoing procedures requiring general anesthesia or deep sedation should inform all care providers of their Zepbound use due to aspiration risk from delayed gastric emptying.
Ozempic-Specific Safety Considerations
Ozempic’s cardiovascular outcomes data — from SUSTAIN-6 in T2D patients with established CV disease — provides a level of safety reassurance in that high-risk population that Zepbound has not yet accumulated. The SUSTAIN-6 trial demonstrated a 26% relative risk reduction in MACE, meaning for T2D patients with prior MI, stroke, or established atherosclerosis, Ozempic’s risk-benefit profile has been formally evaluated in a CVOT in a way Zepbound’s has not yet matched, per the Ozempic prescribing information.
Who Should Choose Which Drug?
The clinical and access data above point to distinct patient profiles for each medication.
Choose Zepbound If:
- Your primary goal is weight loss — Zepbound is the only one of the two drugs that is FDA-approved for this purpose. SURPASS-2 head-to-head data shows tirzepatide 15 mg produces ~6.7 percentage points more weight loss than semaglutide 1 mg at 40 weeks in T2D patients, per ADA SURPASS summary. SURMOUNT-1 data shows up to −20.9% loss in non-diabetic patients, per NEJM 2022, Jastreboff et al.
- You have T2D and want maximum weight loss alongside glycemic control — SURMOUNT-2 showed −14.7% at 15 mg in T2D patients, with 49% achieving normoglycemic HbA1c, per Lancet 2023
- You have moderate-to-severe obstructive sleep apnea with obesity — Zepbound is the first and only FDA-approved medication for this indication, per the Eli Lilly OSA press release
- You are a Medicare beneficiary — the Medicare GLP-1 Bridge (July–December 2026) is available for Zepbound at $50 copayment for the weight management indication; Ozempic is not eligible for this program for obesity, per KFF analysis
- You want commercial insurance coverage for weight management — approximately 43–45% of commercial plans cover Zepbound on-label for obesity; Ozempic’s off-label weight-loss use is typically denied, per Pandameds insurance analysis
Choose Ozempic (or Wegovy) If:
- You have type 2 diabetes and need on-label glycemic management — Ozempic is the FDA-approved and commercially covered option for T2D blood sugar control, with a well-established track record since 2017
- You have established cardiovascular disease with T2D — Ozempic holds an FDA indication for cardiovascular risk reduction based on SUSTAIN-6 MACE reduction data, per the Ozempic prescribing information. Zepbound’s CVOT data is not yet available.
- Your insurer covers Ozempic for T2D but not Zepbound — in this scenario, Ozempic may be the most cost-effective path to a GLP-1 agent, with the understanding that weight loss results will be lower than with tirzepatide
- You would prefer Wegovy (on-label semaglutide for weight management) — if your goal is weight loss and you prefer semaglutide, the correct comparison is Zepbound vs. Wegovy, not Zepbound vs. Ozempic. See our Zepbound vs. Wegovy comparison for that specific analysis, including the SURMOUNT-5 head-to-head results
Neither Drug Is Appropriate If:
- You have a personal or family history of medullary thyroid carcinoma (MTC) or MEN 2
- You are pregnant — both drugs may cause fetal harm; discontinue when pregnancy is recognized
- You are currently taking any other GLP-1 receptor agonist
- You have a known serious hypersensitivity to tirzepatide or semaglutide
Switching Between Zepbound and Ozempic
Switching between these two drugs is medically feasible but requires careful planning and coordination with your prescriber. The key clinical principles:
Switching from Ozempic to Zepbound: Begin Zepbound’s 2.5 mg initiating dose approximately one week after your last Ozempic injection, then re-titrate on the standard Zepbound schedule (2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg, increasing by 2.5 mg every ≥4 weeks), per Zepbound prescribing information. Re-titrating from the initiating dose — rather than attempting to dose-match — allows the GI system to adjust to the different dual-receptor engagement profile.
Switching from Zepbound to Ozempic: Start Ozempic’s 0.25 mg initiation dose approximately one week after the last Zepbound dose and titrate per the standard Ozempic schedule. If the goal is weight management (rather than T2D glycemic control), the more appropriate switch would be to Wegovy at 0.25 mg initiation, since Ozempic is not indicated for weight loss.
Critical rule: These drugs must never be taken simultaneously. Tirzepatide activates the GLP-1R — the same receptor semaglutide targets. Concurrent use creates compounding, unpredictable receptor activation and is explicitly contraindicated, per the FDA Zepbound approval press release.
Insurance transition note: Switching from Ozempic to Zepbound requires a new prior authorization under your Zepbound benefit (if applicable). PA approval for Ozempic under a T2D benefit does not transfer to Zepbound under an anti-obesity medication benefit. Begin the insurance process before your intended switch date — not the day of.
Compounding: What Is and Is Not Available in 2026
The compounding landscape differs meaningfully between tirzepatide and semaglutide — a distinction that matters if you are evaluating lower-cost alternatives.
Tirzepatide (Zepbound): Both 503A (state-licensed compounding pharmacy) and 503B (outsourcing facility) windows for compounding essentially-copy tirzepatide are closed. The 503A enforcement deadline was February 18, 2025; the 503B deadline was March 19, 2025, per the FDA clarification page. As of April 2026, compounded tirzepatide is not legally permissible for general dispensing. Only narrow individualized exceptions apply (documented allergy to branded excipients, specific dose not commercially available). No compounded tirzepatide product is a legitimate substitute for Zepbound.
Semaglutide (Ozempic): The semaglutide compounding window closed later — enforcement deadlines for 503A pharmacies passed April 22, 2025, and for 503B outsourcing facilities, May 22, 2025, per Alston & Bird legal analysis, March 2025. As of April 2026, compounded semaglutide for general dispensing as a cheaper alternative to branded Ozempic or Wegovy is also not legally authorized. Narrow 503A exceptions for documented patient-specific needs remain, but these are not general population offerings.
Any telehealth platform still marketing “compounded Ozempic” or “compounded tirzepatide” as a general cash-pay option in 2026 is not operating within FDA-sanctioned boundaries. The legitimate self-pay paths are LillyDirect for Zepbound and NovoCare for Ozempic.
How to Discuss This With Your Provider
Decision Flowchart: Zepbound vs. Ozempic
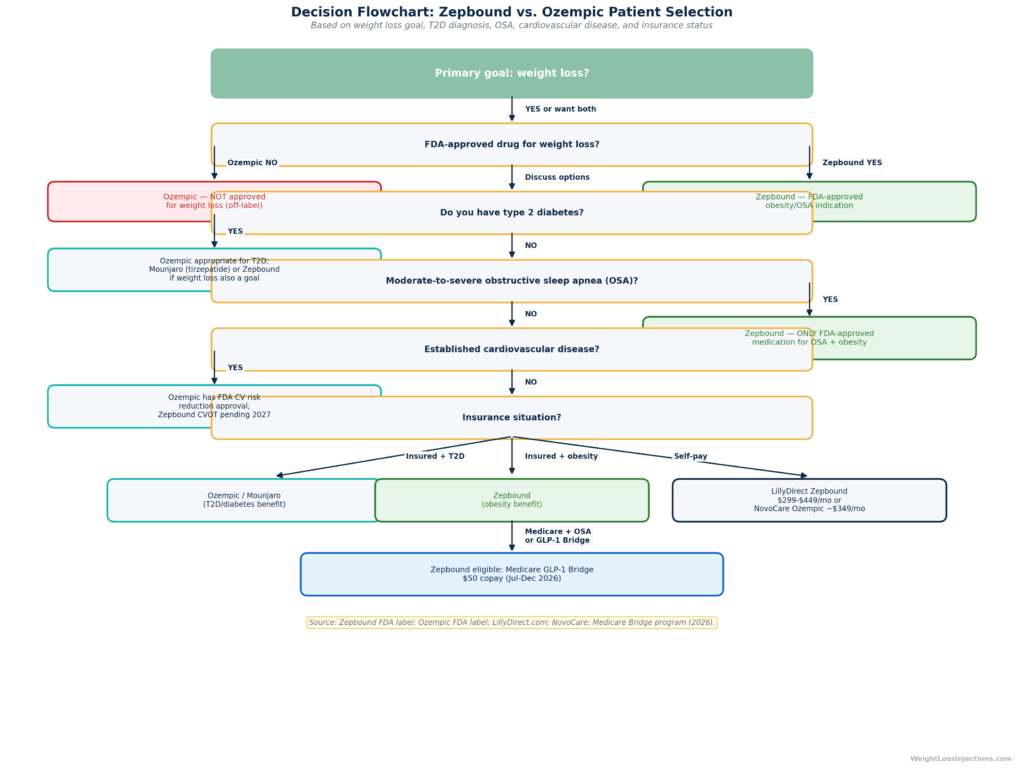
When you bring this question to a provider, the most productive conversation focuses on four variables:
- Your primary medical goals. Weight loss specifically, T2D glycemic control, OSA treatment, or cardiovascular risk reduction — each maps to a different drug and indication.
- Your diagnosis history. T2D, established CVD, OSA, and MTC/MEN 2 history all directly affect which drug is on-label, covered, and safe for you.
- Your insurance situation. Commercial coverage, Medicare, or self-pay each has different cost structures. Your provider can assist with prior authorization paperwork — starting that process before you need the drug avoids delays.
- Your weight-loss goals and timeline. If achieving ≥15–20% body weight loss is the target, the available data consistently favors tirzepatide. If the goal is 5–10% loss as an adjunct to T2D management, semaglutide may be adequate and more easily covered under your existing diabetes benefit.
At WeightLossInjections.com, our licensed providers conduct a full intake evaluation, including BMI, comorbidities, contraindication screening, and insurance review, before making a prescription recommendation. If you want to understand which medication fits your specific profile, take our free eligibility quiz at WeightLossInjections.com and connect with a licensed provider via a virtual consult. No in-person visit is required. Prescription is sent directly to LillyDirect, NovoCare, or the pharmacy of your choice. Our supervised program starts at [$X/month] and includes [service detail].
Our Take at WeightLossInjections.com
Our take at WeightLossInjections.com: Framing this as “Zepbound vs. Ozempic” slightly misidentifies the comparison. Ozempic is a type 2 diabetes drug. Its true comparator for weight loss is Zepbound vs. Wegovy, the on-label semaglutide formulation designed and dosed for obesity management. Patients seeking weight loss via Ozempic are using it off-label, accepting lower-than-maximum semaglutide doses, and facing coverage headwinds that on-label drugs do not encounter.
That said, the practical reality is that millions of patients have been prescribed Ozempic for weight loss, and the off-label use is clinically defensible at appropriate doses under supervised care. The evidence just makes clear that it is not the optimal choice when weight loss is the primary goal: SURPASS-2 shows tirzepatide at 15 mg produces roughly double Ozempic-equivalent semaglutide 1 mg weight loss in a T2D population, and SURMOUNT-1 shows tirzepatide’s ceiling of −20.9% at maximum dose in a non-diabetic population is substantially above what Ozempic’s labeled doses produce. For patients specifically managing T2D who want comprehensive glycemic and weight benefit with the best available evidence, tirzepatide (as Mounjaro for T2D or Zepbound for weight management) is the more efficacious option per the data we have.
The cases where Ozempic genuinely makes sense: patients with established cardiovascular disease who have T2D and need the MACE-reduction evidence base; patients whose insurer covers Ozempic for T2D but not Zepbound under an AOM benefit; and patients who have historically tolerated semaglutide well and have no motivation to switch. Outside those cases, the weight-loss-focused patient is usually better served by Zepbound, and the off-label labeling of Ozempic creates real-world friction, on coverage, on dose, and on indication, that Zepbound does not carry.
Our recommendation: tell your provider your primary goal. If it is weight loss, start the Zepbound eligibility conversation. If it is T2D management, Ozempic (or Mounjaro) is the right on-label path. The drugs are not interchangeable, and the label distinction is not bureaucratic, it reflects real differences in what these drugs were designed, tested, and approved to do.
Frequently Asked Questions
In available direct comparison data (SURPASS-2, 40 weeks, T2D population), tirzepatide 15 mg produced −11.2% average weight loss versus semaglutide 1 mg at −5.7% — approximately double the result at the highest tirzepatide dose. Across all three tirzepatide doses in SURPASS-2 (5, 10, 15 mg), weight loss was statistically superior to semaglutide 1 mg, per ADA SURPASS program summary. The important caveat: SURPASS-2 used semaglutide 1 mg, not its maximum 2 mg dose; and Wegovy’s 2.4 mg (the on-label weight-loss dose of semaglutide) was not the comparator. For weight loss specifically, Zepbound is the FDA-approved drug; Ozempic is not approved for this indication. The correct weight-loss comparator for Zepbound is Wegovy — which was tested head-to-head in SURMOUNT-5 (Zepbound 20.2% vs. Wegovy 13.7% at 72 weeks), per PubMed SURMOUNT-5.
Yes. Zepbound’s FDA weight management indication specifically includes adults with overweight (BMI ≥27) who have at least one weight-related comorbid condition — and type 2 diabetes is an explicitly listed qualifying comorbidity, per the FDA Zepbound approval press release. The SURMOUNT-2 trial, which enrolled 938 adults with T2D, showed tirzepatide 15 mg produced −14.7% weight loss at 72 weeks with 49% of patients reaching normoglycemic HbA1c, per Lancet 2023. Note that tirzepatide also comes as Mounjaro (the T2D-indicated formulation), the same molecule and the same dose range, but with a different approved indication. Your provider will determine which brand and indication is most appropriate based on your diagnosis and insurance situation.
Both Ozempic and Wegovy contain semaglutide, but they are different drugs for regulatory, dosing, and coverage purposes. Ozempic is FDA-approved for type 2 diabetes at doses up to 2 mg weekly. Wegovy is FDA-approved for chronic weight management in adults with obesity or overweight at a 2.4 mg weekly maintenance dose — a higher dose than Ozempic’s label permits. Wegovy also holds additional FDA approvals for cardiovascular risk reduction, MASH, and pediatric obesity (ages 12+). Using Ozempic for weight loss is off-label; Wegovy is the on-label semaglutide formulation for obesity. Commercially, this means insured patients seeking weight-loss drug coverage are steered toward Wegovy, not Ozempic. The FDA Wegovy approval page and Ozempic prescribing information document these separate regulatory designations.
Standard Medicare Part D does not cover either drug for the weight management indication, Medicare is statutorily prohibited from covering drugs used solely for weight loss, per American College of Gastroenterology guidance, April 2025. There are exceptions: Zepbound may be covered under Part D when prescribed for moderate-to-severe OSA; Ozempic may be covered for its T2D and cardiovascular indications; and a temporary Medicare GLP-1 Bridge program (July 1–December 31, 2026) provides Zepbound and Wegovy at a $50 copayment for eligible Part D enrollees with BMI ≥35, or ≥27 with clinical criteria, per KFF analysis. Ozempic does not qualify for the weight-management Bridge program — that coverage applies to on-label anti-obesity medications.
Yes. Telehealth prescribing is well established for Zepbound, and no in-person visit is required to start treatment. A licensed provider conducts a virtual consultation covering your BMI, weight-related comorbidities, contraindication screening, and medical history, then sends a prescription to LillyDirect or a retail pharmacy of your choice. The process typically takes one to several days from intake to prescription dispatch. At WeightLossInjections.com, [service detail] connects you with a licensed clinician for [$X/month], including the initial eligibility evaluation, prescription management, and ongoing clinical check-ins. Note: compounded tirzepatide is not legally available from any pharmacy in 2026 for general use, only FDA-approved Zepbound, per the FDA clarification page.
For most patients: no. Compounded tirzepatide became impermissible following the closure of 503A (February 18, 2025) and 503B (March 19, 2025) windows after the FDA confirmed the tirzepatide shortage was resolved, per the FDA compounding clarification page. Compounded semaglutide followed under separate timelines: 503A enforcement deadline April 22, 2025; 503B May 22, 2025, per Alston & Bird legal analysis. Narrow 503A exceptions exist for documented patient-specific clinical needs (allergy to branded excipients, required dose not commercially available) — but these are not general population alternatives. Any platform marketing “compounded Ozempic” or “compounded Zepbound” to the general public in 2026 is operating outside FDA-sanctioned boundaries. The legal self-pay options are LillyDirect for Zepbound ($299–$449/mo) and NovoCare for Ozempic ($349–$499/mo).
This article is for informational purposes only and does not constitute medical advice. All pricing and regulatory information reflects verified sources as of April 2026; prices and program availability are subject to change. WeightLossInjections.com editorial team reviews content quarterly; last verified April 2026. Consult a licensed provider before starting, changing, or stopping any medication.
